-
Is there any interest in an RSS feed of ChEMBL?

Sometimes, when something great happens, you've just got to find out, or tell the world, straight away, just like those proud fellas in the picture above.
So, would there be an interest in an RSS feed of selected ChEMBL content? The sort of thing that is probably useful would be to have alerts for new bioactivity for an already existing ChEMBL compound, or for an already existing ChEMBL target/assay.
Any comments/mail gratefully received. If there is interest, we'll integrate this into our plans for next year. -
Do you know any compounds that are 3A4 inhibitors and great substrates for other P450s?
 Off work ill at the moment, snotty child on lap, and the new Marvel Avengers film on DVD. Anyway, the opening scene got me thinking, "I wonder if there are any good reversible 3A4 inhibitors that are great substrates for one of the other liver P450s". That tells you how good the movie is.Imagine you've got Drug A, which is a great drug iv, but has poor oral bioavailability due to gut 3A4 metabolism when orally dosed. Now imagine, you co-dose with Drug B, which is a gut-specific 3A4 inhibitor, to improve the bioavailability/reduce efficacious dose of Drug A.So the basic idea is to see if it's possible to improve bioavailability by inhibition of gut wall 3A4 by another drug - of course, the original drug will still probably be good liver 3A4 feedstock as well, but it may be a way of improving of PK for poorly behaved drugs. If that 3A4 inhibitor was also a good substrate for another liver localised P450, like 1A2, 2C9, 2C19, or 2D6, there would be low systemic exposure of this compound, and potential subsequent reduction of DDIs since the 3A4 in the liver would be largely spared, etc. i.e. the gut 3A4 inhibitor had high first pass metabolism, and would in effect be a functional gut-specific 3A4 inhibitor.I guess some of these other liver P450s are polymorphic, so, avoiding 2D6 and 2C19 may be worthwhile.Of course, this is in an area ripe for DDIs, induction of non-linear PK, etc., but if anyone knows of any pre-existing studies, or specific examples of drugs that have something approaching this effect, I'd be really interested. So, if you know any examples, post them in the comments!P.S. A sort of related 'systems biology' view of modulating drug metabolism would involve the use of bacterial glucoronidase inhibitors to reduce enterohepatic recirculation (these would need to stay in the gut and have no systemic exposure). Regorafenib is an example of a drug with potentially serious liver tox. and undergoes enterohepatic recirculation but I don't know if it is glucoronidated, or indeed the route of excretion - but i may well try to find out.
Off work ill at the moment, snotty child on lap, and the new Marvel Avengers film on DVD. Anyway, the opening scene got me thinking, "I wonder if there are any good reversible 3A4 inhibitors that are great substrates for one of the other liver P450s". That tells you how good the movie is.Imagine you've got Drug A, which is a great drug iv, but has poor oral bioavailability due to gut 3A4 metabolism when orally dosed. Now imagine, you co-dose with Drug B, which is a gut-specific 3A4 inhibitor, to improve the bioavailability/reduce efficacious dose of Drug A.So the basic idea is to see if it's possible to improve bioavailability by inhibition of gut wall 3A4 by another drug - of course, the original drug will still probably be good liver 3A4 feedstock as well, but it may be a way of improving of PK for poorly behaved drugs. If that 3A4 inhibitor was also a good substrate for another liver localised P450, like 1A2, 2C9, 2C19, or 2D6, there would be low systemic exposure of this compound, and potential subsequent reduction of DDIs since the 3A4 in the liver would be largely spared, etc. i.e. the gut 3A4 inhibitor had high first pass metabolism, and would in effect be a functional gut-specific 3A4 inhibitor.I guess some of these other liver P450s are polymorphic, so, avoiding 2D6 and 2C19 may be worthwhile.Of course, this is in an area ripe for DDIs, induction of non-linear PK, etc., but if anyone knows of any pre-existing studies, or specific examples of drugs that have something approaching this effect, I'd be really interested. So, if you know any examples, post them in the comments!P.S. A sort of related 'systems biology' view of modulating drug metabolism would involve the use of bacterial glucoronidase inhibitors to reduce enterohepatic recirculation (these would need to stay in the gut and have no systemic exposure). Regorafenib is an example of a drug with potentially serious liver tox. and undergoes enterohepatic recirculation but I don't know if it is glucoronidated, or indeed the route of excretion - but i may well try to find out. -
New Drug Approvals 2012 - Pt. XXI - Regorafenib (Stivarga®)

ATC code: L01XE21
Wikipedia: Regorafenib
On September 27th 2012 the FDA approved Stivarga (Regorafenib) for the treatment of metastatic colorectal cancer who have previously received chemotherapy, anti-EGFR or anti-VEGF therapy.
Colorectal or bowl cancer is one of the most common cancers in the western world, is the third most common cancer in the United States and the second most common cause of cancer deaths in the United Kingdom (according to CRUK). While Five-year survival rates of the primary cancer have been improving due to the availability of targeted therapy, they only extend to about 50%, however, the metastatic disease has poor prognosis. In clinical trials Regorafenib showed statistically significant improvement in survival of patients with metastatic disease as compared to the best standard care alone, with the median survival being extended from 5 to 6.4 months.
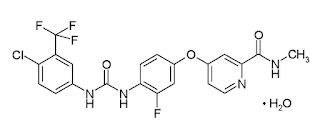
Regorafenib (research code: BAY-73-4506; chembl id :CHEMBL1946170 is a monohydrate and it has a molecular formula C21H15ClF4N4O3 • H2O and a molecular weight of 500.83 (for the mono hydrate) It has very poor water solubility.
Regorafenib is metabolized by CYP3A4 and UGT1A9. The main circulating metabolites of regorafenib measured at steady-state in human plasma are M-2 (N-oxide) and M-5 (N-oxide and N-desmethyl).
Regorafenib has been approved with a boxed warning due to severe hepatotoxicity which can be fatal.
At the clinically active dose, Regorafenib (and its primary active metabolites M-2 and M-5) are multi-kinase inhibitors showing in-vitro activity against RET (P07949), VEGFR1(FLT1, P17948), VEGFR2(KDR, P35968), VEGFR3(FLT4, P35916), KIT(P10721), PDGFR-alpha(P16234), PDGFR-beta(P09619), FGFR1(P11362), FGFR2(P21802), TIE2(Q02763), DDR2(Q16832), Trk2A, Eph2A , RAF1(P04049), BRAF, BRAFV600E(BRAF, P15056) , SAPK2(MAPK11, Q15759), PTK5(FRK, P42685), and ABL1(P00519).
Prescribing information is here.
Stivarga is marketed by Bayer
-
Position in Computational Chemical Biology at Novartis in Cambridge MA

Novartis have a position available in Cambridge MA....
...for a highly motivated scientist in the in silico Lead Discovery group of the Center for Proteomic Chemistry platform. This is an exciting opportunity to perform cutting-edge computational research at their Cambridge USA site. The position will be responsible for the development of robust computational hypothesis with a variety of drug discovery project teams for the purposes of lead discovery, and will apply state of the art computational approaches to elucidate the biological profile of small molecules regarding their targets, off-targets and phenotypic outcome via an in-depth understanding of biological networks, systems biology, bioinformatics and cheminformatics.
Further details are available here. -
Looking for some help on a computational chemistry problem....

I have an interesting little conformational analysis/transition-state problem, that is beyond my zone of competence (no cheeky comments!). It's a really interesting little research problem related to 'click' chemistry - and is probably about a weeks work to someone who knows what they are doing. It's a problem involving conformational analysis for some ~12 heavy atom (CHNO only, no exotics) systems, and then some transition state analysis. To me, it's the sort of thing that needs some MM conformational analysis, followed by MO calculations, and then some thinking through the stability of ground state and transition state forms.
Sorry I can't give explicit details here, but it is a cool idea, and if we can do something good, it will be a good publication (which of course, you would be a co-author on :) ).
So, if you're interested, get in touch.... -
New Drug Approvals 2012 - Pt. XX - Bosutinib (Bosulif®)
 On September 4th, the FDA approved bosutinib (marketed as Bosulif) for the treatment of patients with previously treated Philadelphia Chromosome-Positive (Ph+) Chronic Myelogenous Leukemia (CML - cancer of the white blood cells).
On September 4th, the FDA approved bosutinib (marketed as Bosulif) for the treatment of patients with previously treated Philadelphia Chromosome-Positive (Ph+) Chronic Myelogenous Leukemia (CML - cancer of the white blood cells).
Chronic myelogenous leukemia is one of the four most common types of leukemia and is often associated with treatment with imatinib (CHEMBL941) as an initial therapy. However, approximately one-third of patients do not achieve an optimal response with this standard treatment. In such cases, second generation Tyrosine Kinase Inhibitors are required, but only half of the treated patients show acceptable outcomes. The patients with poor responses to either of these treatments have now the possibility to receive bosutinib (CHEMBL288441) as alternative therapy.
As suggested by the '-tinib' prefix (USAN stem), bosutinib is a protein kinase inhibitor (ATC:L01XE14). The molecule has a calculated logP of 3.88 and relative molecular weight of 530.4. It is therefore too heavy to satisfy the rule of five (maximum molecular weight of 500). The drug is taken orally with food with a recommendation of 500 mg per day. BOSULIF is available as tablet of 100 and 500 mg.
Canonical SMILES: COc1cc(Nc2c(cnc3cc(OCCCN4CCN(C)CC4)c(OC)cc23)C#N)c(Cl)cc1Cl
Standard InChI: 1S/C26H29Cl2N5O3/c1-32-6-8-33(9-7-32)5-4-10-36-25-13-21-18(11-24(25)35-3)26(17(15-29)16-30-21)31-22-14-23(34-2)20(28)12-19(22)27/h11-14,16H,4-10H2,1-3H3,(H,30,31)
Standard InChI Key: UBPYILGKFZZVDX-UHFFFAOYSA-N
As the drug is metabolized by CYP3A4 (UNIPROT:P08684) it could therefore interact with other compounds acting on the enzyme, such as P-glycoprotein inhibitors or CYP3 inducers. Proton pump inhibitors can also decrease the drug concentration in the human body.
Most common adverse reactions (incidence greater than 20%) are diarrhea, nausea, thrombocytopenia, vomiting, abdominal pain, rash, anemia, pyrexia and fatigue.
The product website is www.bosulif.com, full prescribing information is here. -
TIMBAL - A database of Protein-Protein Interactions

TIMBAL is a database containing small molecules that modulate protein-protein interactions (PPIs). It was first created in 2008, by manually curating information extracted from relevant scientific publications. An analysis of the data was published in 2009, (Higueruelo et al, 2009). The growth of data in the past years makes hand-curated databases a phenomenally time-consuming task. The maintenance of TIMBAL is done now through automated searches on the ChEMBL database (currently using ChEMBL_14). The list of known PPI targets (thank you!) and its orthologs has been translated into UniProt codes. These codes are then used in ChEMBL for searching small molecule data related to these proteins in binding assays with confidence that the assay is directly assigned to a single protein or its homolog. Currently the database has 4,681 data points from more than three thousand small molecules across 27 targets. The database also refers to 600 PDB entries related to these targets.
Check it out! -
New Drug Approvals 2012 - Pt. XIX - Enzalutamide (Xtandi capsulesTM)

On August 31, the FDA approved Enzalutamide for the treatment of castration-resistant prostate cancer. Prostate cancer affects predominantly men aged 50 years and older and is the sixth most frequent source of cancer-related deaths in men world-wide.
The prostate is a gland located below the bladder that surrounds the urethra and secretes simple sugars, citrate, zinc and other constituents of liquid semen. Prostate cancer in many cases has only mild symptoms, even without treatment. Prostate cancer can be detected by measuring concentrations of the biomarker prostate specific antigen. Its progression stage is assessed by the widely established Gleason grading scheme. In many cases it is sufficient to monitor cancer progression without treatment.
For aggressive tumors, various treatment options are available and include surgery, irradiation, cryosurgery, chemotherapy and hormonal therapy. Hormonal therapy relies on the tumor's dependence on androgen signalling, which can be ablated using the antiandrogens flutamide (CHEMBL806) and bicalutamide (CHEMBL409). However, after about two to three years, many prostate cancers become refractory to hormone therapy, even though they still rely on androgen signalling. These so-called castration resistant cancers can be treated with docetaxel (CHEMBL92) and, as a second line of defense, the newly approved Enzalutamide.
Enzalutamide and its primary metabolite N-desmethyl enzalutamide competitively inhibit androgen binding to the androgen receptor (Uniprot P10275).
Enzalutamide is a small molecule with molecular weight 464.44 and calculated logP of 3.88. It is practically insoluble in water and is administered in liquid-filled soft gelatin capsules.
IUPAC: 4-{3-[4-cyano-3-(trifluoromethyl)phenyl]-5,5 dimethyl-4-oxo-2-sulfanylideneimidazolidin-1-yl}-2-fluoro-N-methylbenzamide
SMILES: CNC(=O)c1ccc(N2C(=S)N(c3ccc(C#N)c(C(F)(F)F)c3)C(=O)C2(C)C)cc1F
InChI=1S/C21H16F4N4O2S/c1-20(2)18(31)28(12-5-4-11(10-26)15(8-12)21(23,24)25)19(32)29(20)13-6-7-14(16(22)9-13)17(30)27-3/h4-9H,1-3H3,(H,27,30)
InChIKey=WXCXUHSOUPDCQV-UHFFFAOYSA-N
Enzatulamide is administered in a daily dose of 160mg, which equates to four 40mg capsules. It has a Cmax of 16.6µg/mL that is reached after about one hour and is 97% bound to plasma proteins.
Enzatulamide is metabolised primarily by CYP2C8 (P10632) and CYP3A4 (P08684). A major metabolite, N-desmethyl enzalutamide has similar bioactivity as enzatulamide.
Adverse reactions include asthenia/fatigue, back pain, diarrhea and others.
Enzatulamide is marketed by Medivation under the trade name Xtandi.







