I missed this for some reason - two new higher resolution structures of squid rhodopsin. Anyway, it's been processed and will be added to the usual places later today. The reference is:
%T Crystallographic analysis of the primary photochemical reaction of squid rhodopsin.
%A Murakami M
%A Kouyama T
%J J. Mol. Biol.
%D 2011
%V 413
%P 615-627
It sometimes takes me a little bit of time to understand and appreciate concepts that others pick up easily; one of these areas is around pathways and networks. The diagrams are great, and make great visual images. I have one on my office wall. It seems the more connections there are, the better - but can people understand these big messes as opposed to a simplified critical path map? There are now some great tools to explore these networks, things like cytoscape, and the annotation of these pathway diagrams is clearly valuable. One of the best books I’ve read of the broad field was the early book by Barabasi - ‘Linked’, but this is quite old now, and there has been a lot of progress.
I was at an excellent workshop this week at the NIH in Bethesda, and I was fortunate enough to participate in a specific workshop session around networks and perturbagens. This had some of the real thought-leaders of the field in, and it was great to put a face to some of the names from papers I had read. I do have a couple of things I still haven’t worked out yet, so I thought I’d try and write down what they are, and pose some questions to the ChEMBL-oggers for clarification, trigger some discussion, chat about examples, etc.
Fundamentally I feel that these networks must be most valuable when they are based on physical interactions, these must give better insight into mechanism. However, it is really common to have links between genes on the basis of transcriptional co-regulation, and given that there appears to be no standards for the display of physical compared to virtual interactions, I find working out what on earth is going on with a diagram really complex. Are there standard ways of representing the classes of interaction (physical obligate, physical transient, transcriptional, etc)?
Are there much literature connected to a domain level annotation of the networks; for example, prothrombin, the gla-domains, the kringles and the serine proteinase domain, etc, they all have different partners, and their partners usually bind at different surfaces. In terms of using the networks to think about regulation, surely the definition or annotation of the eptopes/binding sites must be essential in order to mine these networks?
How do people deal with mapping the effect of purturbagens onto these networks - the whole of pharmacology and drug discovery is built around quantitation of dose response, and there must be ways of showing the reconfiguration of networks as concentration of a perturbagen is raised?
The stability/stoichiometry of the components of these networks seems to be typically ignored - homo-oligomerisation is surely a valid class of interaction, and a lot of biology is based around concentration dependent oligomerisation events. Also people typically don’t seem to worry too much about stable complexes, versus more dynamic more highly kinetic interactions. Is this as big an issue as I think it might be?
How do researchers define the boundaries of these networks, is there an accepted convention to stop these networks growing too large - so how do people do pruning?
Is there anyway that people validate these networks, a sort of statistic that measures the statistical support for a particular topology, or fragility of the particular rendering of the network.?
Finally, probably again related to the validation of these networks and their usefulness in quantitative biology - do people routinely map available assays across the nodes, of course these could span many connected nodes, but mapping these pathways to bioassays must be a useful thing? This would clearly be a cool thing to try and do with ChEMBL.
So, I’m sure I just haven’t read the literature, so let me know - or if any of the points above are interesting research areas get in touch!
Sorry if these posts are a little off normal topic. But the majority of the member of the EBI's team for Movember assembled yesterday for a 'before' photo. Just look at all those baby faces, look at all those chins!
There is a great meeting being held in Oxford just after the Christmas break (specifically on the 5th and 6th January 2012), it's organised by the Structural Genomics Consortium, one of the longest existing advocates of Open Science in Drug Discovery.
The EBI has a team entered for the annual Movember fund raising event - this is focussed on raising money for 'male cancers' - testicular and prostate. The team is called The Bioinformoustachians!, so please consider sponsoring us over the coming month. Of course, as well as raising money for a serious cause, there will be some fun along the way as well. Watch over the next few days, as the full team signs up - we're gonna raise Loadsamoney (hopefully).
For those unfamiliar with the idea - participants are clean shaved at the start and grow a moustache throughout the month gaining sponsorship for looking stylish/silly.
The team webpage on the movember website is here. Please consider donating, and help us, together, make a difference.
On October 24th, the FDA approved Clobazam (Tradename: OnfiTM; Research Code: RU-4723), a GABAA receptor agonist, for the adjunctive treatment of seizures associated with Lennox-Gastaut syndrome (LGS) in patients aged two years or older.
Lenox-Gastaut syndrome is a rare and severe form of epilepsy that is typically diagnosed in childhood and often persists into adulthood. LGS accounts for 1-4% of childhood epilepsies, and it is associated with multiple types of seizures, as well as, daily periods of frequent seizures.
Clobazam decreases the frequency of the LGS seizures by potentiating GABAergic neurotransmission, trough the binding of the GABAA receptor at the benzodiazepine site.
GABAA receptor is a protein complex of five subunits (mainly α2β2γ) located in the synapses of neurons. All GABAA receptors contain an ion channel that conducts chloride ions across neuronal cell membranes and two binding sites for the neurotransmitter GABA, while a subset of GABAA receptor complexes also contain a single binding site for benzodiazepines, also referred to as benzodiazepine receptors (BzR). Benzodiazepines, like clobazam, bind at the interface of the α and γ subunits on the GABAA receptor. Once bound to the benzodiazepine receptor, the benzodiazepine ligand locks the benzodiazepine receptor into a conformation in which it has a greater affinity for the GABA neurotransmitter. This increases the frequency of the opening of the associated chloride ion channel and hyperpolarizes the membrane of the associated neuron. The inhibitory effect of the available GABA is potentiated, leading to sedatory and anxiolytic effects.
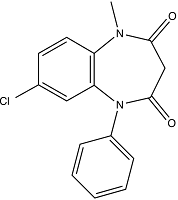
Clobazam (IUPAC: 7-chloro-1-methyl-5-phenyl-1,5-benzodiazepine-2,4-dione; SMILES: CN1C(=O)CC(=O)N(c2ccccc2)c3cc(Cl)ccc13; PubChem: 2789; Chemspider: 2687; ChEMBLID: CHEMBL70418; Standard InChI Key: CXOXHMZGEKVPMT-UHFFFAOYSA-N) has a molecular weight of 300.7 Da, two hydrogen bond acceptors, no hydrogen bond donors, and has an ALogP of 2.74. Clobazam is a benzodiazepine derivative, a large and well established class of pharmacologically active compounds. So far, it is the only marketed 1,5-benzodiazenpine, being prefered over the 1,4-benzodiazepines already in the market: clonazepam and nitrazepam.
Clobazam is available as oral tablets of 5, 10 and 20mg, and the recommend daily dose is twice the amount of the tablets according to body weight. It has an apparent volume of distribution of 100L at steady state, and its relative bioavailability compared to an oral solution is 100%. The major metabolite of Clobazam is N-desmethylclobazam, which has about 1/5 of the activity of clobazam. Both compounds bind to human plasma proteins (80-90% and 70% respectively). The estimated mean elimination half-life (t1/2) is approximately 36-42 hr for clobazam and 71-82 hr for the active metabolite.
Clobazam is mainly metabolised by CYP3A4 and to a lesser extent by CYP2C19 and CYP2B6. In vitro metabolism studies demonstrate that clobazam and its active metabolite induce CYP3A4 activity in a concentration-dependent manner. N-desmethylclobazam is extensively metabolised by the polymorphic CYP2C19, therefore, dosage in patients who are known CYP2C19 poor metabolisers may need to be adjusted. For further drug-drug interactions please refer to the full prescribing information.
Clobazam has been granted an orphan drug designation because it is intended to treat a condition that affects fewer than 200,000 people.
The license holder for OnfiTM is Lundbeck, and the full prescribing information can be found here.
Although clobazam has just been approved in the United States, it has been marketed outside of the US for several years under various brand names, including Frisium® and Urbanyl®, both licensed by Sanofi-Aventis. A full list of brand names can be found here.
On October 14th, 2011 FDA announced the approval of Deferiprone (trade name: FerriproxTM) for the treatment of iron overload which is potentially fatal in patients with thalassemia. Deferiprone is an oral iron chelating agent, binding excess iron in the blood and thus making it available to excretion from the body.
Thalassaemia is a inherited (mostly autosomal recessive) blood disease that can lead to anemia by causing the formation of abnormal hemoglobin molecules not able to properly bind and release oxygen.
Thalassaemia (OMIM: 141800 (α-) / 141900 (β-)) is sub-classified according to which of the subunits of the hetero-tetrameric (2α/2β, UniProt: P69905 / P68871) hemoglobin is affected, contrary to sickle-cell anaemia (OMIM: 603903) which results exclusively from a specific mutation in the β subunit. The primary treatment of thalassaemia major, the severe form of β-thalassaemia, requires frequent blood transfusions to establish stable levels of functional hemoglobin but results in high levels of iron accumulating and impairing organ function. Thus, the secondary treatment aims on reducing the toxic iron levels by binding excess iron utilizing an iron chelating agent such as Deferoxamine (ChEMBL ID: CHEMBL556) requiring parenteral administration; Deferiprone has the desirable property of being orally available.
Deferiprone (3-hydroxy-1,2-dimethylpyridin-4(1H)-one, canonical SMILES: CN1C=CC(=O)C(=C1C)O, Standard InChI: InChI=1S/C7H9NO2/c1-5-7(10)6(9)3-4-8(5)2/h3-4,10H,1-2H3 , ChEMBL ID: CHEMBL556, CAS number: 30652-11-0, PubChem: CID 2972, ChemSpider: 2866) is a very simple synthetic small molecule with molecular weight of 139.152 Da, it has no rotatable bonds, two hydrogen bond acceptors, one hydrogen bond donor, ALogP of -0.14 and is thus fully rule-of-five compliant.
Ferriprox is dosed as 500 mg tablets and administred orally three times daily in doses of 25 mg/kg to 33 mg/kg body weight (rounded to the nearest half-tablet), resulting in a daily molar dose of ~38-50 mmol for a 70 kg individual. Common adverse reactions include chromaturia, nausea, vomiting and abdominal pain, among others. Ferriprox is not suitable for pregnant or nursing women. Ferriprox reaches a maximum concentration (Cmax) of 20 mcg/mL, has an elimination half life (t1/2) of 1.9 hours and is excreted renally. The volume of distribution is 1.6 L/kg and 1 L/kg in thalassaemia patients and healthy subjects, respectively. Peak serum concentrations are reached 2 to 4 hours after administration.
Ferriprox has been issued a boxed warning for its potential to cause agranulocytosis/neutropenia, hematological disorders characterized by abnormally low numbers of white blood cells potentially leading to serious infections and death.
Ferriprox is marketed and has been developed by Apotex.
The full prescribing information can be found here. Prior to its approval in North America, Ferriprox has been approved and available in Europe and Asia for several years - approval in North America had been delayed considerably by safety concerns brought forward by a clinical researcher formerly involved in the clinical studies.



 Sorry if these posts are a little off normal topic. But the majority of the member of the EBI's team for Movember assembled yesterday for a 'before' photo. Just look at all those baby faces, look at all those chins!
Sorry if these posts are a little off normal topic. But the majority of the member of the EBI's team for Movember assembled yesterday for a 'before' photo. Just look at all those baby faces, look at all those chins! There is a great meeting being held in Oxford just after the Christmas break (specifically on the 5th and 6th January 2012), it's organised by the Structural Genomics Consortium, one of the longest existing advocates of Open Science in Drug Discovery.
There is a great meeting being held in Oxford just after the Christmas break (specifically on the 5th and 6th January 2012), it's organised by the Structural Genomics Consortium, one of the longest existing advocates of Open Science in Drug Discovery.


 Deferiprone (3-hydroxy-1,2-dimethylpyridin-4(1H)-one, canonical SMILES: CN1C=CC(=O)C(=C1C)O, Standard InChI: InChI=1S/C7H9NO2/c1-5-7(10)6(9)3-4-8(5)2/h3-4,10H,1-2H3 , ChEMBL ID: CHEMBL556, CAS number: 30652-11-0, PubChem: CID 2972, ChemSpider: 2866) is a very simple synthetic small molecule with molecular weight of 139.152 Da, it has no rotatable bonds, two hydrogen bond acceptors, one hydrogen bond donor, ALogP of -0.14 and is thus fully rule-of-five compliant.Ferriprox is dosed as 500 mg tablets and administred orally three times daily in doses of 25 mg/kg to 33 mg/kg body weight (rounded to the nearest half-tablet), resulting in a daily molar dose of ~38-50 mmol for a 70 kg individual. Common adverse reactions include chromaturia, nausea, vomiting and abdominal pain, among others. Ferriprox is not suitable for pregnant or nursing women. Ferriprox reaches a maximum concentration (Cmax) of 20 mcg/mL, has an elimination half life (t1/2) of 1.9 hours and is excreted renally. The volume of distribution is 1.6 L/kg and 1 L/kg in thalassaemia patients and healthy subjects, respectively. Peak serum concentrations are reached 2 to 4 hours after administration.Ferriprox has been issued a boxed warning for its potential to cause agranulocytosis/neutropenia, hematological disorders characterized by abnormally low numbers of white blood cells potentially leading to serious infections and death.Ferriprox is marketed and has been developed by Apotex.The full prescribing information can be found here. Prior to its approval in North America, Ferriprox has been approved and available in Europe and Asia for several years - approval in North America had been delayed considerably by safety concerns brought forward by a clinical researcher formerly involved in the clinical studies.
Deferiprone (3-hydroxy-1,2-dimethylpyridin-4(1H)-one, canonical SMILES: CN1C=CC(=O)C(=C1C)O, Standard InChI: InChI=1S/C7H9NO2/c1-5-7(10)6(9)3-4-8(5)2/h3-4,10H,1-2H3 , ChEMBL ID: CHEMBL556, CAS number: 30652-11-0, PubChem: CID 2972, ChemSpider: 2866) is a very simple synthetic small molecule with molecular weight of 139.152 Da, it has no rotatable bonds, two hydrogen bond acceptors, one hydrogen bond donor, ALogP of -0.14 and is thus fully rule-of-five compliant.Ferriprox is dosed as 500 mg tablets and administred orally three times daily in doses of 25 mg/kg to 33 mg/kg body weight (rounded to the nearest half-tablet), resulting in a daily molar dose of ~38-50 mmol for a 70 kg individual. Common adverse reactions include chromaturia, nausea, vomiting and abdominal pain, among others. Ferriprox is not suitable for pregnant or nursing women. Ferriprox reaches a maximum concentration (Cmax) of 20 mcg/mL, has an elimination half life (t1/2) of 1.9 hours and is excreted renally. The volume of distribution is 1.6 L/kg and 1 L/kg in thalassaemia patients and healthy subjects, respectively. Peak serum concentrations are reached 2 to 4 hours after administration.Ferriprox has been issued a boxed warning for its potential to cause agranulocytosis/neutropenia, hematological disorders characterized by abnormally low numbers of white blood cells potentially leading to serious infections and death.Ferriprox is marketed and has been developed by Apotex.The full prescribing information can be found here. Prior to its approval in North America, Ferriprox has been approved and available in Europe and Asia for several years - approval in North America had been delayed considerably by safety concerns brought forward by a clinical researcher formerly involved in the clinical studies.





