-
Internship - Scientific Data Visualisation

We are looking for an intern for one month to design a new poster on drugs and their targets. We published a poster a few years ago, and now we want to make a new poster, built around pharmacological action and drug types. We are looking for someone with good aesthetic judgement, ideally a long-standing interest in scientific data visualisation and experience is network visualisation using tools such as Cytoscape. Familiarity with Adobe Illustrator on Mac OsX is essential. If you are interested, please get in touch.
The EMBL-EBI pays a standard stipend to all interns. -
New Drug Approvals 2011 - Pt. XXIII Ticagrelor (BrilintaTM)

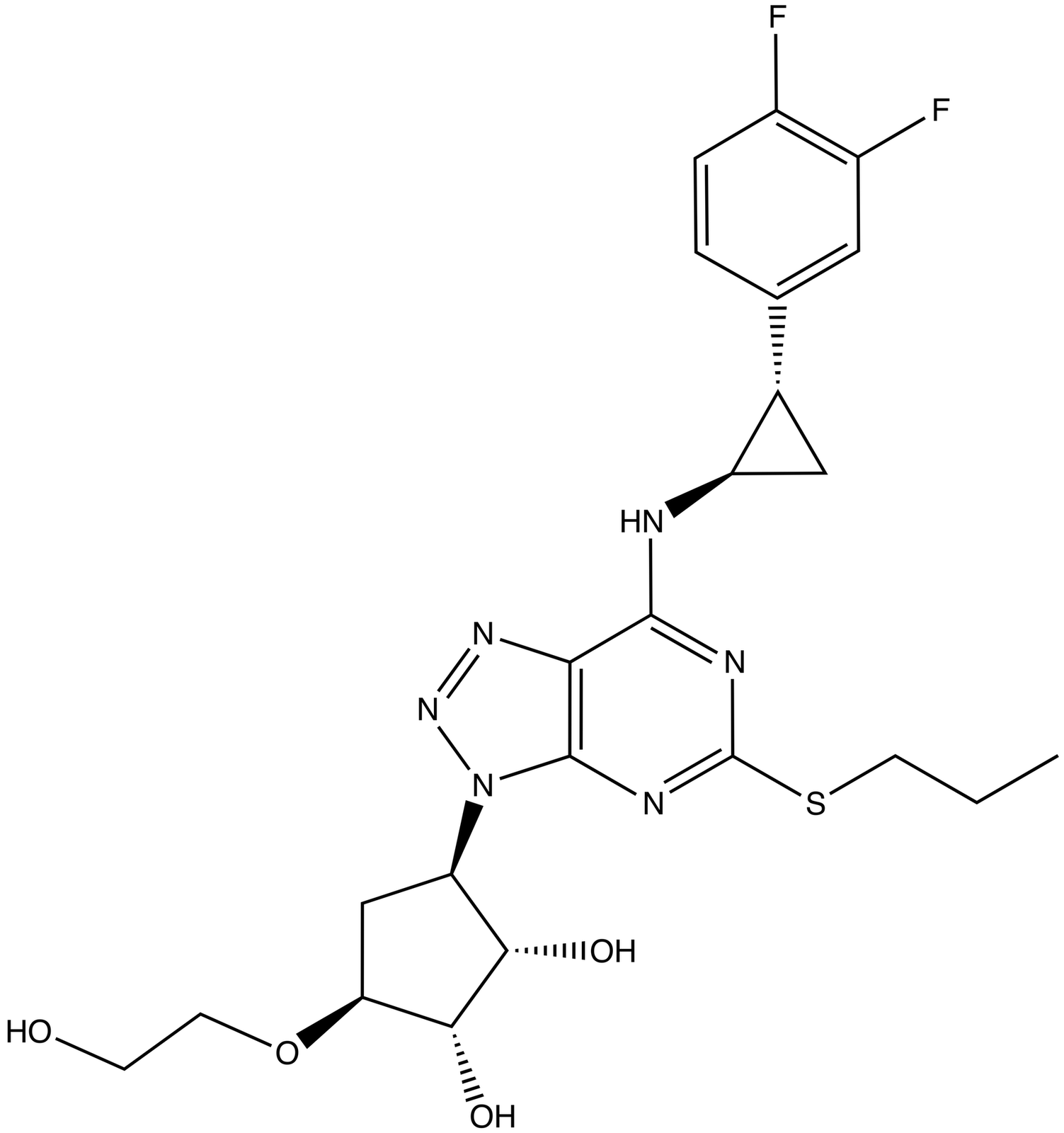
On July 20th, the FDA approved Ticagrelor (Tradename: Brilinta; Research Code: AZD-6140, NDA 022433), a purinergic receptor P2Y12 platelet antagonist indicated to reduce the rate of thrombotic cardiovascular events in patients with acute coronary syndrome (ACS).
Acute coronary syndrome is often the initial presentation of an individual manifesting coronary artery disease (CAD). ACS can present as unstable angina, non-ST elevation myocardial infarction, or ST elevation myocardial infarction. Typically, ACS begins with the rupture or erosion of a vulnerable plaque in a coronary artery, which results in the exposure of elements under the endothelial layer, such as collagen or von Willebrand factor, to circulating blood. These ligands trigger a series of responses, including platelet adhesion, activation, and aggregation.
Ticagrelor reduces the thrombotic risk in ACS by blocking the P2Y12 receptor on the platelet surface. This drug is the first reversible drug for the Purinergic receptor P2Y12, and prevents the binding of ADP by inducing a reversible conformational change. It is thus an allosteric antagonist. Inhibition of the signal transduction results in reduced exposure of fibrinogen-binding sites to the GP IIb/IIIa receptor and thereby impairment of platelet aggregation. Similarly to other approved drugs to treat ACS, such as Prasugrel (Tradename: Effient; ChEMBL ID: CHEMBL1201772) and contrary to clopidogrel (Tradename: Plavix; ChEMBL ID: CHEMBL1771) and ticlopidine (Tradename: Triclid (Discontinued); ChEMBL ID: CHEMBL833), ticagrelor is not a pro-drug, although its active metabolite (AR-C124910XX) has a comparable potency.
Purinergic receptor P2Y12 (Uniprot accession: Q9H244; ChEMBL ID: CHEMBL2001; OMIM: 609821) is a Rhodopsin-like receptor and therefore it is a member of the G-protein coupled receptor 1 family. The sequence of P2Y12 is:
>P2Y12 MQAVDNLTSAPGNTSLCTRDYKITQVLFPLLYTVLFFVGLITNGLAMRIFFQIRSKSNFI IFLKNTVISDLLMILTFPFKILSDAKLGTGPLRTFVCQVTSVIFYFTMYISISFLGLITI DRYQKTTRPFKTSNPKNLLGAKILSVVIWAFMFLLSLPNMILTNRQPRDKNVKKCSFLKS EFGLVWHEIVNYICQVIFWINFLIVIVCYTLITKELYRSYVRTRGVGKVPRKKVNVKVFI IIAVFFICFVPFHFARIPYTLSQTRDVFDCTAENTLFYVKESTLWLTSLNACLDPFIYFF LCKSFRNSLISMLKCPNSATSLSQDNRKKEQDGGDPNEETPM
There are no known 3D structures for this protein, but there are now several relevant homologous structures of other members of the family (see here for a current list of rhodopsin-like GPCR structures).
The -grel- or -grel USAN/INN stem covers primarily platelet P2Y12 receptor antagonists. Ticagrelor is the first reversible inhibitor of this class, and ticlopidine, clopidogrel and prasugrel all bind irreversibly to P2Y12. Other compounds in this class in late stage clinical development/registration include Portola Pharmaceuticals' elinogrel (Research code: PRT 060128), The Medicines Company's cangrelor (Research code: AR-C69931XX), and the Inspire Pharmaceuticals' regrelor (Research code: INS50589). Others at earlier stages of development include Arena Pharmaceuticals' temanogrel (Research code: APD791).

Ticagrelor (IUPAC: (1S,2S,3R,5S)-3-[7-[[(1R,2S)-2-(3,4-difluorophenyl)cyclopropyl]amino]-5-propylsulfanyltriazolo[4,5-d]pyrimidin-3-yl]-5-(2-hydroxyethoxy)cyclopentane-1,2-diol; SMILES: CCCSC1=NC2=C(C(=N1)N[C@@H]3C[C@H]3C4=CC(=C(C=C4)F)F)N=NN2[C@@H]5C[C@@H]([C@H]([C@H]5O)O)OCCO; PubChem:9871419; Chemspider:8047109, ChEMBLID: CHEMBL398435, Standard InChI Key:OEKWJQXRCDYSHL-FNOIDJSQSA-N) has a molecular weight of 522.6 Da, contains 4 hydrogen bond donors, 8 hydrogen bond acceptors, and has an ALogP of 2.37. Ticagrelor contains six defined stereocenters. Ticagrelor is a cyclopentyl-triazolo-pyrimidine and these agents are relatively resistant to enzymatic degradation by ectonucleotidases. Ticagrelor has clear structural resemblance to adenosine, the endogenous ligand for P2Y12, we have classified it as a natural product-derived small molecule drug.
Ticagrelor is available as an oral film-coated tablets of 90 mg, and the recommend daily dose is 180 mg (equivalent to 34.4 umol). It has an apparent volume of distribution of 88 L and its mean absolute bioavailability is 36% (range 30%-42%). Absorption of ticagrelor occurs with a median tmax of 1.5 h, and the formation of its active metabolite occurs with a median tmax of 2.5 hr. Both compounds are extensively bound to human plasma proteins (>99%). The mean plasma half-life (t1/2) is approximately 7 hours for ticagrelor and 9 hr for the active metabolite.
Ticagrelor is mainly metabolised by CYP3A4 and to a lesser extent by CYP3A5; therefore, other therapeutic agents that inhibit or induce these enzymes may alter their therapeutic effect or lead to adverse DDIs. In vitro metabolism studies demonstrate that ticagrelor and its active metabolite are inhibitors of the P-gp transporter. Ticagrelor has been studied in ACS in combination with aspirin. Maintenance doses of aspirin above 100 mg decreased the effectiveness of ticagrelor.
Ticagrelor has been issued with a black box warning because, like other antiplatelet agents, it can cause potentially fatal bleeding.
The license holder for Ticagrelor is AstraZeneca, and the full prescribing information can be found here. Ticagrelor was approved in the EU in 2010 and is commercialised under the tradename Brilique. The European SPC can be found here. -
2011 (to date) USANs by molecular class

So, we're about half way through the year, and just update the July 2011 USANs - here is a graph of the USAN molecular class for all names published this year. This set of USANs, will, on average, suffer about 80% attrition and the survivors will be launched in ca. three or four years time. (See previous posts for some details on this). So, this 'year class' is a snapshot of types the drugs to come in 2014-2015.
There are 83 drugs in this 2011 set (actually, I need to find out the official dating of USAN assignment, since some published in 2011 are assigned 2010 dates). All the supporting data for this is contained in the blog posts, and it took about five minutes to assemble from this source, but if you'd like a spreadsheet mail me. Small molecules are in various shades of blue, Biologicals in various shades of green, or pink or purple; Protein type biologicals are subdivided into a series of intuitive classes (see earlier posts on drug taxonomy for details).

It's interesting to note that the majority of the molecules are still synthetic small molecules, two thirds in fact, while only a quarter are 'biologicals'. Looking at quite a lot of data like this makes me query, a little, the well forecasted dominance of biologicals; what really is the data that shows a forthcoming dominance of biologicals, on what timescales, etc. Of course, there is a big difference between economic dominance, and simple counts of novel molecular entities (NME); and biological therapies are more arguably premium priced. However, I think the NME is a pretty good metric for underlying innovation. There are also some interesting differences and similarities in attrition between small molecules and biologicals - small molecules are directed to a different set of targets to biologicals, and many of these targets are already clinically validated. Currently biologicals are directed against more unvalidated targets, and so attrition risk is different between small molecules and biologicals. Our initial analyses suggest that the overall attrition is similar between these two sets (so it's not likely that although a quarter of the class of 2011 USANs are biologicals they will all survive to market.
I have a beach holiday coming up soon, on the delightful south Hampshire coast, and plan to do some more analysis on these USAN datasets, assuming there is wifi on the beach.... -
July 2011 USANS

The July 2011 USANs have just been published.
USAN Research Code Structure Drug Type Drug Class Target alisporivir
DEB-025, Debio-025
Natural product-derived small molecule Therapeutic cyclophilins efinaconazole KP-103 
Synthetic small molecule Therapeutic C. albicans 14-alpha demethylase esomeprazole strontium FM-0F67 
Synthetic small molecule Therapeutic gastric H+/K+ ATPase ixmyelocel-T Cell-based therapy Therapeutic n/a mapracorat ZK-245186 
Synthetic small molecule Therapeutic glucocorticoid receptor obinutuzumab Ro-5072759, huMAB , GA-101, Afutuzumab monoclonal antibody Therapeutic CD-20 olodaterol, olodaterol hydrochloride BI-1744 
Synthetic small molecule Therapeutic Beta-2 adrenergic receptor teriflunomide HMR-1726 
Synthetic small molecule Therapeutic DHODH -
New Drug Approvals 2011 - Pt. XXII Indacaterol Maleate (ArcaptaTM)

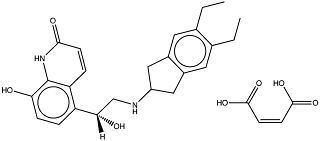
ATC Code: R03AC18On July 1, the FDA approved indacaterol maleate (NDA 022383) for the long-term treatment of patients with chronic obstructive pulmonary disease (COPD) a chronic and serious disease involving restriction of full lung function. The narrowing of airways of COPD is irreversible, and follows inflammation in the lung, believed to be linked to environmental pollutants such as tobacco smoke, workplace dusts and urban air pollution. Indacaterol maleate is administered as an aerosol through a dry powder inhaler and carries a boxed warning for asthma-related death and is not indicated for the treatment of asthma.
The active ingredient of indacaterol maleate is indacaterol (ChEMBL: 1095777) an agonist of the beta-2 adrenergic receptor (Uniprot: P07550, ChEMBL: 210) with measured EC50 of 11nM. Indacaterol exerts its effect through activation of the beta-2 adrenergic receptor, leading to smooth muscle relaxation and a widening of bronchioli in the lungs. Activation of the beta-2 adrenergic receptor stimulates the intracellular adenyl cyclase and increases cAMP levels, which in turn leads to a reduction of the level of calcium ions inside smooth muscle cells. Other long acting beta-adrenoceptor agonists (LABA) such as salmeterol, formoterol and bambuterol entered the market during the 1980s. The duration of action of these earlier compounds is 12 hours, while for indacaterol it is 24 hours.
Multiple crystal structures of the beta-2 adrenergic receptor now exist (PDBe: 2R4R, 2R4S, 2RH1, 3D4S, 3KJ6, 3NY8, 3NY9, 3NYA, 3P0G, 3PDS), a nano-body stabilized structure of the receptor in its activated form is shown below (PDBe: 3p0g).
Indacaterol (IUPAC: (R)-5-(2-((5,6-diethyl-2,3-dihydro-1H-inden-2-yl)amino)-1-hydroxyethyl)-8-hydroxyquinolin-2(1H)-one, SMILES: CCc1cc2CC(Cc2cc1CC)NC[C@H](O)c3ccc(O)c4NC(=O)C=Cc34 , InChI: 1S/C24H28N2O3/c1-3-14-9-16-11-18(12-17(16)10-15(14)4-2)25-13-22(28)19-5-7-21(27)24-20(19)6-8-23(29)26-24/h5-10,18,22,25,27-28H,3-4,11-13H2,1-2H3,(H,26,29)/t22-/m0/s1, ChemSpider: 5293751, ChEMBL: 1095777) is a is a synthetic small molecule drug with one chiral center. It has a molecular weight of 392.5 Da and calculated LogP of 3.93. Indacaterol has 4 hydrogen bond acceptors and 4 hydrogen bond donors and therefore fully complies with Lipinski's rule of five. The picture below shows both the active ingredient, indacaterol, and maleate.
The USAN stem name -terol indicates that indacaterol is a phenethylamine derivative bronchodilator. Other -terols include salmeterol, formoterol, bambuterol, vilanterol, milveterol and levalbuterol.
 Indacaterol's bioavailability after inhalation is (at the recommended dose range of 75-150 µg) is 43-45% and the volume of distribution (Vd) is between 2.36 and 2.56 L.kg-1 and a clearance (CL) of about 20L.hr-1. Steady-state of Indacaterol levels is reached within 12 to 15 days. Plasma protein binding (ppb) of the dosed drug is 95.1-96.2%. Excretion of indacaterol is mainly through the fecal route, either as the parent compound (54% of the dose) or hydroxylated metabolite (23% of the dose).
Indacaterol's bioavailability after inhalation is (at the recommended dose range of 75-150 µg) is 43-45% and the volume of distribution (Vd) is between 2.36 and 2.56 L.kg-1 and a clearance (CL) of about 20L.hr-1. Steady-state of Indacaterol levels is reached within 12 to 15 days. Plasma protein binding (ppb) of the dosed drug is 95.1-96.2%. Excretion of indacaterol is mainly through the fecal route, either as the parent compound (54% of the dose) or hydroxylated metabolite (23% of the dose).
Indacaterol maleate is administered once daily as an aerosol containing 75-150 µg of active ingredient from a powder inhaler.
The full prescribing information can be found here.
Indacaterol maleate was approved by the European commission in 2009 and is marketed in Europe as Onbrez. In the US, indacaterol maleate will be marketed by Novartis under the trade name Arcapta. -
New Drug Approvals 2011 - Pt. XXI Rivaroxaban (XareltoTM)

On July 1st, FDA approved Rivaroxaban (trade name: Xarelto, Research code: BA-59-7939, NDA 022406), an anti-coagulant to prevent deep vein thrombosis (DVT) in patients with knee or hip replacement surgery. Rivaroxaban is the first orally applied direct inhibitor of Factor Xa (FXa), a key regulatory of the coagulation cascade. In DVT, a blood clot is formed which can dislodge and travel to the lungs, causing pulmonary embolism which can be potentially fatal.
Factor Xa (EC number 3.4.21.6, UniProt ID P00742, OMIM 613872) is a serine endopeptidase, cleaving prothrombin into its active form, thrombin, which then activates further downstream factors which ultimately lead to platelet activation and fibrin formation, clotting the damaged blood vessels. The sequence of Factor X is
>Factor X MGRPLHLVLLSASLAGLLLLGESLFIRREQANNILARVTRANSFLEEMKKGHLERECMEE TCSYEEAREVFEDSDKTNEFWNKYKDGDQCETSPCQNQGKCKDGLGEYTCTCLEGFEGKN CELFTRKLCSLDNGDCDQFCHEEQNSVVCSCARGYTLADNGKACIPTGPYPCGKQTLERR KRSVAQATSSSGEAPDSITWKPYDAADLDPTENPFDLLDFNQTQPERGDNNLTRIVGGQE CKDGECPWQALLINEENEGFCGGTILSEFYILTAAHCLYQAKRFKVRVGDRNTEQEEGGE AVHEVEVVIKHNRFTKETYDFDIAVLRLKTPITFRMNVAPACLPERDWAESTLMTQKTGI VSGFGRTHEKGRQSTRLKMLEVPYVDRNSCKLSSSFIITQNMFCAGYDTKQEDACQGDSG GPHVTRFKDTYFVTGIVSWGEGCARKGKYGIYTKVTAFLKWIDRSMKTRGLPKAKSHAPE VITSSPLK
Factor X itself is synthesized as an inactive precursor, and is further processed into a mature form, consisting of a light and an "activated" heavy chain (=FXa, residues 235-488, bold in the above sequence, carrying a trypsin-like domain, Pfam PF00089) (green and red in the below picture, respectively). There is a plethora of experimentally solved structures available for FXa, and also a holostructure of FXa in complex with Rivaroxaban, PDBe:2w26.

Rivaroxaban (ChEMBL ID 198362, ATC code B01AX06, PubChem CID 6433119) has molecular weight of 435.9 Da, an ALogP of 1.8, 5 rotatable bonds, 6 hydrogen bond acceptors, 1 hydrogen bond donor, and is thus fully Rule-of-Five compliant. It is dosed as a pure (S)-enantiomer. Canonical Smiles, Smiles=Clc1ccc(s1)C(=O)NC[C@H]2CN(C(=O)O2)c3ccc(cc3)N4CCOCC4=O, Standard InChi, InChI=1S/C19H18ClN3O5S/c20-16-6-5-15(29-16)18(25)21-9-14-10-23(19(26)28-14)13-3-1-12(2-4-13)22-7-8-27-11-17(22)24/h1-6,14H,7-11H2,(H,21,25)/t14-/m0/s1. Rivaroxaban is known to have a sub-nanomolar (0.7 nM) IC50 to the active site of human FXa.

Xarelto is administered orally as a 10 mg tablet once daily for 12 or 35 days (after knee/hip replacement surgery, respectively), yielding ~23 umol of active substance per single dose. Most relevant risks connected to Xarelto treatment are serious and fatal bleeding.
It has been given a boxed warning for spinal/epidural hematoma in surgical settings. It has not been tested in pregnant women, nursing mothers, or pediatric settings; majority of participants in clinical trials were 65 years and over, and the efficacy of Xarelto in the elderly was found to be similar to that seen in younger patients. The effect of Xarelto lasts 8-12 hours, but FXa activity stays depleted during 24 hours, so a once-daily dose is sufficient.
It has high (80-100%) bioactivity and is rapidly absorbed, reaching Cmax at 2 to 4 hours. Its volume is distribution is Vss=50 L. Little metabolism is observed for rivaroxaban, with the majority of the dose excreted unchanged.
The USAN/INN name stem, -xaban of rivaroxaban, designates a FXa inhibitor. Alternative anticoagulants, inhibiting FXa indirectly, include Heparin (ChEMBL ID 526514), an activator of Antithrombin, which itself is a FXa inactivator; Warfarin (ChEMBL ID 1464), a vitamin K antagonist, vitamin K being required for FXa biosynthesis. However, numerous other direct FXa inhibitors are currently being developed, e.g. Apixaban (BMS-562247-01, ChEMBL ID 231779), Betrixaban (PRT-054021, ChEMBL ID 512351), Edobaxan (Du-176b), Eribaxaban (PD-348292), Fidexaban (ZK-807834), Otamixaban (XRP-0673), YM-150, YM-466, Letaxaban (TAK-442), and GW-813893.
Xarelto has been developed by Bayer Schering AG. In US, it will be marketed by Janssen Pharmaceuticals, Inc.
The product website can be found here, the full prescribing information, here. -
New Drug Approvals 2011 - Pt. XX azficel-T (laVivTM)

On June 21st 2011, the FDA approved azficel-T (trade name: laViv) for the aesthetic treatment of moderate to severe nasolabial fold wrinkles in adults ("smile lines"). laViv is an autologous cell therapeutic, consisting of fibroblasts (cells which can produce collagen) which are produced from a biopsy of post-auricular tissue by proliferation in vitro, and re-injected into the nasolabial folds to improve their cosmetic appearance. With increasing age, nasolabial folds can become more pronounced, caused by habitual facial expressions (i.e. laughing), and a decline of collagen production.
Alternative non-drug treatments include liposuction and facelift. After biopsy, dermal fibroblasts are expanded using standard tissue-culture procedures until a sufficient amount of cells for re-injection is obtained. This process takes 11-22 weeks. laViv is provided in two vials of approximately 18 million fibroblasts in 1.2 mL suspension and should be administered in three sessions at 3-6 weeks intervals by injection at 0.1 mL per linear centimeter of nasolabial fold wrinkle. The mechanism by which laViv works is not known.
In two clinical trials, the efficacy of azficel-T has been evaluated based on a five-point Subject Wrinkle Assessment scale, and additionally by physicians employing a six-point Evaulator Wrinkle Severity Assessment, and considered successful if a two-point improvement post- compared to pre-treatment was achieved. In both studies, the Subject Wrinkle Assessment for the group using laViv (57%/45%) was significantly improved as compared to the vehicle control group (30%/18%); equally, the Physician Wrinkle Assessment indicated an improvement of the condition using laViv (33%/19% as compared to 7% for both control groups). To avoid immune reactions, the identity of donor and recipient has to be assured.
Common adverse reations are injection-site reactions such as redness, bruising, swelling, and pain. Pediatric safety and efficacy have not been established; clinical studies lack sufficient number of subjects in geriatric or non-White population. Efficacy of the product beyond six months has not been established. laViv has been developed by Fibrocell Technologies.
The product website can be found here, full prescribing information, here. -
Paper: PSICQUIC and PSISCORE: accessing and scoring molecular interactions

To study proteins in the context of a cellular system, it is essential that the molecules with which a protein interacts are identified and the functional consequence of each interaction is understood. A plethora of resources now exist to capture molecular interaction data from the many laboratories generating such information, but whereas such databases are rich in information, the sheer number and variability of such databases constitutes a substantial challenge in both data access and quality assessment to the researchers interested in a specific biological domain.
The paper is available here, and here is the PSICQUIC registry.
%T PSICQUIC and PSISCORE: accessing and scoring molecular interactions %A B. Aranda %A H. Blankenburg %A S. Kerrien %A F.S.L. Brinkman %A A. Ceol %A E. Chautard %A J.M. Dana %A J. De Las Rivas %A M. Dumousseau %A E. Galeota %A A. Gaulton %A J. Goll %A R.E.W. Hancock %A R. Isserlin %A R.C. Jimenez %A J. Kerssemakers %A J. Khadake %A D.J. Lynn %A M. Michaut %A G. O'Kelly %A K. Ono %A S. Orchard %A C. Prieto %A S. Razick %A O. Rigina %A L. Salwinski %A M. Simonovic %A S. Velankar %A A. Winter %A G. Wu %A G.D. Bader %A G. Cesareni %A I.M. Donaldson %A D. Eisenberg %A G.J. Kleywegt %A J. Overington %A S. Ricard-Blum %A M. Tyers %A M. Albrecht %A H. Hermjakob %J Nature Methods %V 8 %P 528–529 %D 2011 %O doi:10.1038/nmeth.1637






{kind=link}