On June 15th 2011, the FDA has approved Belatacept (trade name: Nulojix; Research Code: BMS-224818), a selective T-cell (lymphocyte)costimulation blocker indicated for phophylaxis of organ rejection in adult patients receiving a kidney transplant. Belatacept is approved for use in combination with other immunosuppressants, specifically basiliximab, mycophenolate mofetil and corticosteroids.
Belatacept is a potent antagonist that inhibits T-lymphocyte activation by binding to the B7-ligands, namely CD80 (Uniprot: P33681; Pfam: PF08205, PF07686) and CD86 (Uniprot: P42081; Pfam: PF07686), present on antigen-presenting cells, and thereby blocking interaction with CD28 (Uniprot: P10747; Pfam: PF07686), the receptor of these two ligands. This interaction provides a costimulary signal necessary for full activation of T-lymphocytes. Activated T-cells are the predominant mediators of immunologic rejection. In vitro, Belatacept inhibits T-cell proliferation and the cytokinesinterleukin-2, interferon-γ, interleukin-4 and TNF-α.
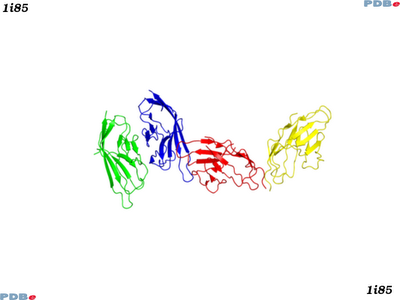
There are some protein structures known for the B7-ligands, CD80 and CD86. Here are two typical entries for CD80 (PDBe:1i8l) and CD86 (PDBe:1i85) in complex with CTLA-4.
Belatacept is derived from Abatacept (trade name: Orencia; approved in 2005 for the treatment of rheumatoid arthritis, ChEMBLID: CHEMBL1201823), a soluble fusion protein that consists of the extracellular domain of the human cytotoxic T-lymphocyte antigen-4 (CTLA-4; Uniprot: P16410; Pfam: PF07686), linked to a modified Fc (hinge-CH2-CH3 domains) portion of human immunoglobulin G1 (CTLA4-Ig). CTLA-4 is similar to the T-cell costimulatory protein CD28, and both molecules bind to CD80 and CD86 on antigen-presenting cells. However, CTLA-4 transmits an inhibitory signal to T-cells, whereas CD28 transmits a stimulatory signal. Although Abatacept binds to the B-7 ligands with higher affinity when compared with CD28, it has never reached the market as an organ transplantation therapy due to the fact that it does not completely and equally block of the costimulation pathway (the difference in antagonistic effect to CD80 compared with CD86 is a 100-fold decrease in affinity to the CD86). Given this, Belatacept was developed by altering two amino acids in the B-7 ligand-binding portion of the Abatacept molecule (a leucine and an alanine were replaced by a glutamic acid and a tyrosine, respectively). These modifications have resulted in a 4-fold increase in binding affinity to the CD86 and a 2-fold increase in CD80 binding affinity in comparison to Abatacept. Also, it has been shown that, in vitro, this increase in binding affinity to the B-7 ligands resulted in a 10-fold increase in inhibiting T-cell activation when compared with Abatacept.
Other immunosuppressive therapies to treat transplant rejection are available on the market and these include calcineurin inhibitors, such as Tacrolimus (ChEMBLID: CHEMBL1237096), mTOR inhibitors, such as Everolimus (ChEMBLID: CHEMBL1201755), anti-proliferatives, such as Mycophenolic acid (ChEMBLID: CHEMBL866), corticosteroids, such as Hydrocortisone (ChEMBLID: CHEMBL389621) and antibodies, such as Basiliximab (ChEMBLID: CHEMBL1201439) and Rituximab (ChEMBLID: CHEMBL1201576).
Belatacept recommended dosage is a 10 mg/kg intravenous infusion on days 1 (day of transplantation) and 5, end of weeks 2, 4, 8, and 12 after transplantation in the initial phase, followed by a maintenance phase of 5 mg/kg at the end of week 16 after transplantation and every 4 weeks thereafter. The molecular weight of Belatacept is approximately 90 kDa. After a 10 mg/kg intravenous infusion at week 12, Belatacept has a volume of distribution (Vd) of 0.11 L/kg, a systemic clearance (CL) of 0.49 mL/h/kg and a terminal half-life (t1/2) is 9.8 days. The full prescribing information can be found here.
Another GPCR paper published - this time for the human Histamine H1 receptor - the target of a large number of anti-inflammatory drugs. The structure is complexed with Doxepin, a ligand showing very broad pharmacology. Link to the paper is here.
This makes a total of eight sequence distinct (or seven paralogous) rhodopsin-like GPCRs in the public domain. These are:
The structure is available on-line as PDBe:3rze, as for many other GPCR structures, it is an engineered lysozyme chimera, and diffracts to 3.1Å.
%T Structure of the human histamine H1 receptor complex with doxepin
%J Nature
%D 2011
%A T. Shimamura
%A M. Shiroishi
%A S. Weyand,
%A H. Tsujimoto
%A G. Winter
%A V. Katritch
%A R. Abagyan
%A V. Cherezov
%A W. Liu
%A G.W. Han
%A T. Kobayashi
%A R.C. Stevens
%A S. Iwata
%O doi:10.1038/nature10236
On June 10th, FDA approved ezogabine (trade name Potiga, NDA 022345) to treat seizures associated with epilepsy in adults. However, before being launched, Potiga waits categorised by the Drug Enforcement Agency (for review under the Controlled Substances Act) before formal marketing can proceed.
Epilepsy is a chronic neurological disorder involving a variety of symptoms caused by abnormal electrical activity in the brain. Episodic bouts ('seizures') can potentially be controlled by medication - however, for around 1 in 3 patients, this can not achieved satisfactorily with current medication. Ezogabine (ChEMBLID:41355) represents a novel approach, being the first anticonvulsant to specifically target neuronal potassium channels.
The molecular targets of ezogabine are KCNQ/Kv7 potassium channels; by stabilizing their open conformation, the drug reduces their excitability. It shares its mode of action with the structurally very similar non-opioid analgesic Flupiritine (ChEMBLID:255044). There are numerous other anticonvulsant drugs approved, such as Carbamazepine (ChEMBLID:108), or Lamotrigine (ChEMBLID:741), two sodium channel blockers.
Its name stem, -gab-, designates it a GABA mimetic (γ-Aminobutyric acid, ChEMBL ID 96, the predominant inhibitory neurotransmitter in the mammalian central nervous system). For a substance to be GABAergic, there is no need to directly compete with GABA, or to bind to the GABA receptor. However, there is evidence that ezogabine directly interacts with the GABAA receptor, acting as an allosteric agonist, synergetically increasing GABA binding, thereby excerting a sedative effect additionally to its primary target, KCNQ.
The main molecular target of ezogabine are the human KCNQ2 and -3 potassium channels (UniProt O43526 and O43525, respectively) - according to a patch clamp assay, it has 1.3 uM affinity for the murine KCNQ2 ortholog (see also ref).There are no experimental structures available for members of the KCNQ protein family, although there are X-Ray structures for other potassium channels.
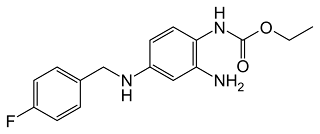
Ezogabine (canonical smiles CCOC(=O)Nc1ccc(NCc2ccc(F)cc2)cc1N , standard InChI InChI=1S/C16H18FN3O2/c1-2-22-16(21)20-15-8-7-13(9-14(15)18)19-10-11-3-5-12(17)6-4-11/h3-9,19H,2,10,18H2,1H3,(H,20,21)) has 6 rotatable bonds, a molecular weight of 303.3 Da, 3 hydrogen bond donors, 2 hydrogen bond acceptors, and is thus fully Rule-of-Five compliant.
Ezogabin has moderately high bioavailability (50-60%), a high volume of distribution (6.2 L/kg) and a terminal half-life of 8 to 11 hours. Potiga tablets are administered three times daily. Ezogabine has a number of potentially severe adverse effects, such as urinary retention, and psychiatric symptoms such as new or intensification of depression, anxiety, psychosis, and in rare cases suicidal thoughts.
Potiga has been developed by Valeant and will be marketed by GSK.
We are starting to plan a few things, and one of these is to provide links through to the sources of physically available compounds for ChEMBL. To help us, here's a few questions - I tried to set up an online poll, but lost the will to live with all the spam on polls that is out there.
Here are the questions:
Is integration of available compounds in ChEMBL a good idea?
Should we integrate available compounds via current informatics resources (e.g. ZINC, ChemSpider)?
Should we set up a small set of available compounds from actual suppliers (e.g. NCGC, MolPort, Prestwick, ChemDiv, Tocris, etc. etc.). If so what suppliers should we use?
If you want to contribute, free to mail if you have any specific ideas, or can help us out on this.
Not Moon Safari but Kinase SARfari! There are a lot of changes to the interface and integration of data, and also oodles more data (104% more) contained in the latest release. These include:
Unified SARREGNOs to CHEMBL IDs (also Assay & Doc ids).
Updated assays, activities and compounds from ChEMBL_10.
Added 30 non-human kinase domains.
Calculated site similarity distances and neighbourhood density (ND) scores between all kinase domains.
Added Drug Icons into the interface.
Added links to ChEMBL Target/Doc/Assay Report Cards.
There are two group leader positions currently listed at the recruitment pages for the Heidelberg site for EMBL. Due to the goofy web recruitment system we have, I can't give a link to the jobs themselves, but you should be able to find them from here.
Areas of interest for one of these posts include:
structural bioinformatics (e.g. modeling of protein complexes and their interactions and/or dynamics in a cellular context).
image analysis/visualization (e.g. reading out data from GFP screens, E-tomograms or visualizing a virtual cell atlas).
We are involved in a fascinating collaboration withProf. Aroon Hingoranifrom the Clinical Epidemiology Dept of UCL Division of Medicine - working with clinical data (phenotype and GWAS) to identify new approaches to the treatment of cardiovascular disease (drug reuse, patient stratifcation, etc.). Further details of the position arehere. Closing date is June 24th 2011. Cool passport eh?


 Belatacept is derived from Abatacept (trade name: Orencia; approved in 2005 for the treatment of rheumatoid arthritis, ChEMBLID: CHEMBL1201823), a soluble fusion protein that consists of the extracellular domain of the human cytotoxic T-lymphocyte antigen-4 (CTLA-4; Uniprot: P16410; Pfam: PF07686), linked to a modified Fc (hinge-CH2-CH3 domains) portion of human immunoglobulin G1 (CTLA4-Ig). CTLA-4 is similar to the T-cell costimulatory protein CD28, and both molecules bind to CD80 and CD86 on antigen-presenting cells. However, CTLA-4 transmits an inhibitory signal to T-cells, whereas CD28 transmits a stimulatory signal. Although Abatacept binds to the B-7 ligands with higher affinity when compared with CD28, it has never reached the market as an organ transplantation therapy due to the fact that it does not completely and equally block of the costimulation pathway (the difference in antagonistic effect to CD80 compared with CD86 is a 100-fold decrease in affinity to the CD86). Given this, Belatacept was developed by altering two amino acids in the B-7 ligand-binding portion of the Abatacept molecule (a leucine and an alanine were replaced by a glutamic acid and a tyrosine, respectively). These modifications have resulted in a 4-fold increase in binding affinity to the CD86 and a 2-fold increase in CD80 binding affinity in comparison to Abatacept. Also, it has been shown that, in vitro, this increase in binding affinity to the B-7 ligands resulted in a 10-fold increase in inhibiting T-cell activation when compared with Abatacept.
Belatacept is derived from Abatacept (trade name: Orencia; approved in 2005 for the treatment of rheumatoid arthritis, ChEMBLID: CHEMBL1201823), a soluble fusion protein that consists of the extracellular domain of the human cytotoxic T-lymphocyte antigen-4 (CTLA-4; Uniprot: P16410; Pfam: PF07686), linked to a modified Fc (hinge-CH2-CH3 domains) portion of human immunoglobulin G1 (CTLA4-Ig). CTLA-4 is similar to the T-cell costimulatory protein CD28, and both molecules bind to CD80 and CD86 on antigen-presenting cells. However, CTLA-4 transmits an inhibitory signal to T-cells, whereas CD28 transmits a stimulatory signal. Although Abatacept binds to the B-7 ligands with higher affinity when compared with CD28, it has never reached the market as an organ transplantation therapy due to the fact that it does not completely and equally block of the costimulation pathway (the difference in antagonistic effect to CD80 compared with CD86 is a 100-fold decrease in affinity to the CD86). Given this, Belatacept was developed by altering two amino acids in the B-7 ligand-binding portion of the Abatacept molecule (a leucine and an alanine were replaced by a glutamic acid and a tyrosine, respectively). These modifications have resulted in a 4-fold increase in binding affinity to the CD86 and a 2-fold increase in CD80 binding affinity in comparison to Abatacept. Also, it has been shown that, in vitro, this increase in binding affinity to the B-7 ligands resulted in a 10-fold increase in inhibiting T-cell activation when compared with Abatacept. 

 The June 2011 USANs have been published.
The June 2011 USANs have been published.