-
Webinar: Accessing ChEMBL Web Services via Workflow Tools
-
New Drug Approvals 2012 - Pt. XVI - Aclidinium bromide (TudorzaTM PressairTM)

On July 23th, the FDA approved Aclidinum bromide (Tradename: Tudorza PressairTM; Research Codes: LAS-34273, LAS W-330), a muscarinic acetylcholine M3 receptor antagonist, for the long-term maintenance treatment of bronchospasm associated with chronic obstructive pulmonary disease (COPD).
Chronic obstructive pulmonary disease (COPD) is characterised by the occurrence of chronic bronchitis or emphysema, a pair of commonly co-existing diseases of the lungs in which the airways become narrowed. Bronchial spasms, a sudden constriction of the muscles in the walls of the bronchioles, occur frequently in COPD.
Aclidinum bromide is a long-acting antimuscarinic agent that through the inhibition of the muscarinic acetylcholine M3 receptors present in the airway smooth muscle, leads to bronchodilation, and consequently eases the symptoms of COPD.
The muscarinic acetylcholine M3 receptor (Uniprot: P20309, ChEMBL: CHEMBL245) belongs to the G-protein coupled receptor (GPCR) type 1 family, and binds the endogenous neurotransmitter acethylcoline. Since it is coupled to a Gq protein, its inhibition leads to a decrease of intracellular calcium levels, and consequently smooth muscle relaxation.
>ACM3_HUMAN Muscarinic acetylcholine receptor M3 MTLHNNSTTSPLFPNISSSWIHSPSDAGLPPGTVTHFGSYNVSRAAGNFSSPDGTTDDPL GGHTVWQVVFIAFLTGILALVTIIGNILVIVSFKVNKQLKTVNNYFLLSLACADLIIGVI SMNLFTTYIIMNRWALGNLACDLWLAIDYVASNASVMNLLVISFDRYFSITRPLTYRAKR TTKRAGVMIGLAWVISFVLWAPAILFWQYFVGKRTVPPGECFIQFLSEPTITFGTAIAAF YMPVTIMTILYWRIYKETEKRTKELAGLQASGTEAETENFVHPTGSSRSCSSYELQQQSM KRSNRRKYGRCHFWFTTKSWKPSSEQMDQDHSSSDSWNNNDAAASLENSASSDEEDIGSE TRAIYSIVLKLPGHSTILNSTKLPSSDNLQVPEEELGMVDLERKADKLQAQKSVDDGGSF PKSFSKLPIQLESAVDTAKTSDVNSSVGKSTATLPLSFKEATLAKRFALKTRSQITKRKR MSLVKEKKAAQTLSAILLAFIITWTPYNIMVLVNTFCDSCIPKTFWNLGYWLCYINSTVN PVCYALCNKTFRTTFKMLLLCQCDKKKRRKQQYQQRQSVIFHKRAPEQAL
There is one partially resolved 3D structure for this protein (2CSA), but there are now several relevant homologous structures of other closely related members of the family (see here for a current list of rhodopsin-like GPCR structures).
The -ium USAN/INN stem covers quaternary ammonium compounds. Members of these class include for example tiotropium bromide (ChEMBL ID: CHEMBL1182657), and ipratropium bromide (ChEMBL ID: CHEMBL1615433, which are also anthicholinergic drugs approved for the treatment of COPD.

Aclidinum bromide (IUPAC: [1-(3-phenoxypropyl)-1-azoniabicyclo[2.2.2]octan-3-yl]2-hydroxy-2,2-dithiophen-2-ylacetate bromide; Canonical smiles (for active quaternary amine): OC(C(=O)O[C@H]1C[N+]2(CCCOc3ccccc3)CCC1CC2)(c4cccs4)c5cccs5 ; PubChem: 11467166; Chemspider: 9609381; ChEMBLID: CHEMBL1194325; Standard InChI Key: ASMXXROZKSBQIH-VITNCHFBSA-N) is a synthetic quaternary ammonium compound with one chiral center, a molecular weight of 484.7 Da, 7 hydrogen bond acceptors, 1 hydrogen bond donor, and has an ALogP of 3.4. The compound is therefore fully rule-of-five compliant.
Aclidinum bromide is available as a dry powder inhaler and the recommended daily dose is two oral inhalations of 400 mcg. It has an apparent volume of distribution of 300 L following intravenous administration of 400 mcg, and its absolute bioavailability is approximately 6%. The estimated effective half-life of Aclidinum (t1/2) is 5 to 8 hours.
The major route of metabolism for aclidinum bromide is non-enzymatic and esterases-mediated hydrolysis, being rapidly and extensively converted to its alcohol and dithienylglycolic acid derivatives, neither of which binds to muscarinic receptors - this leads to very low systemic exposure of the active aclidinium species. Excretion of aclidinium bromide is mainly through the urine (54 - 65%) and faeces (20 - 30%), where only 1% is excreted as unchanged aclidinium. The total clearance is approximately 170 L/h after an intravenous dose of aclidinium bromide in young healthy volunteers.
The license holder for TudorzaTM PressairTM is Forest Pharmaceuticals, and the full prescribing information can be found here. -
What have Natural Products ever done for us?
There's a very accessible article (subscription required) on plant derived natural products in Science recently - this is in the context of understanding and exploiting the biosynthetic pathways to discover new natural products and then engineering new systems to make these or better variants of them; Synthetic Biology.%A V. De Luca %A V. Salim %A S.M. Atsumi %A F. Yu %T Mining the biodiversity of plants: A revolution in the making %J Science %D 2012 %V 336 %P 1658-1661
Table 1 (itself adapted from I. Raskin et al., Trends Biotechnol. 20, 522 (2002)) is interesting and worthy of note (reproduced here without permission ;) ) and lists the most commercially important natural products, lots of 'toxins' in there (e.g. digoxin, taxol, atropine), and some goofy things that we wouldn't normally think of as therapeutic drugs (e.g. nicotine, cocaine). These have a net value of $25 bn per year (although it's unclear if that figure is US only, or how cocaine is 'valued'). They make the claim that 'two-thirds of new drugs in the past 25 years have originated from the discovery of particular secondary metabolites derived from natural biodiversity' - our analysis doesn't support anything like that number, unless the most rose-tinted spectacles are used in the analysis, however, it would be fascinating to see a properly presented case for this number. However, a great orientation to the exciting area of secondary metabolites, and a good pointer to a set of molecules that can successfully modulate 'difficult' targets.
-
Some more ways to access ChEMBL

There's now a BioRuby API for ChEMBL, written by the excellent Mitsuteru Nakao (@32nm on twitter). Bio-chembl is a bioruby plugin built on top of the ChEMBL REST web services - https://github.com/nakao/bio-chembl
Of course, there is also the pychembl project in Python from Marcus Sitzmann of the NCI. - https://github.com/markussitzmann/pychembl
And I've just been reminded of the R ChEMBL package from Rajarshi Guha - https://github.com/rajarshi/chemblr
However, the real mark of success will be when we get a ChEMBL f77 library! -
Science, Technology, Engineering and Mathematics training in the UK

The Select Committee on Science and Technology, part of the UK Government, today published a report into training in Science, Technology, Engineering and Mathematics (STEM). To me this is a real curates egg, parts excellent, parts a little wooly and imprecisely argued. -
New Drug Approvals 2012 - Pt. XV - Carfilzomib (KyorolisTM )

ATC Code: L01XX
Wikipedia: Carfilzomib
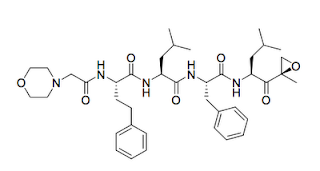
Carfilzomib is a chirally defined modified tetrapeptidyl epoxide substrate analogue with a molecular weight of 719.9. The molecular formula is C40H57N5O7. (SMILES= O=C(N[C@H](C(=O)N[C@H](C(=O)N[C@H(C(=O)N[C@H](C(=O)[C@@]1(OC1)C)CC(C)C)Cc2ccccc2)CC(C)C)CCc3ccccc3)CN4CCOCC4)
Cmax and AUC following a single intravenous dose of 27 mg/m2 was 4,232 ng/mL and 379 ng.hr/mL, respectively. The mean steady-state volume of distribution of a 20 mg/m2 dose of carfilzomib was 28 L. Carfilzomib was rapidly and extensively metabolised, via peptidases and epoxide hydrolyses - i.e. non-CYP mediated metabolism. After intravenous administration of ≥ 15 mg/m2, carfilzomib was rapidly cleared from the systemic circulation with a half-life of ≤ 1 hour.
Carfilzomib is a second generation, non-competitive, irreversible proteasome inhibitor. It contains the unusual (for drugs) epoxide group responsible for the irreversible binding to the target. It is differentiated from the first generation proteasome inhibitor bortezomib (boron-based) in this irreversible inhibition mechanism, which is believed to contribute to overcoming bortezomib resistance. Additionally, clinical trials have showed that carfilzomib is associated with fewer incidences of Peripheral Neuropathy (NP) (incidence reported 14% of patients with 1% having Grade 3 NP) in comparison with bortezomib (36% and 24% Grade 3). Epoxides are quite reactive, and can react with many proteins in a biological system.
The molecular target for carfilzomib is the 20S catalytic core of the large multi-protein complex - the proteasome. Specifically, it binds to the N-terminal threonine-containing active site of the endopeptidase proteasome subunit beta type-7 (Uniprot: Q99436).
The amino acid sequence is:
>sp|Q99436|PSB7_HUMAN Proteasome subunit beta type-7 OS=Homo sapiens GN=PSMB7 PE=1 SV=1 MAAVSVYAPPVGGFSFDNCRRNAVLEADFAKRGYKLPKVRKTGTTIAGVVYKDGIVLGAD TRATEGMVVADKNCSKIHFISPNIYCCGAGTAADTDMTTQLISSNLELHSLSTGRLPRVV TANRMLKQMLFRYQGYIGAALVLGGVDVTGPHLYSIYPHGSTDKLPYVTMGSGSLAAMAV FEDKFRPDMEEEEAKNLVSEAIAAGIFNDLGSGSNIDLCVISKNKLDFLRPYTVPNKKGT RLGRYRCEKGTTAVLTEKITPLEIEVLEETVQTMDTS
Prescribing information had be found here.
The licence holder is Onyx Pharmaceuticals and the product website is www.kyprolis.com -
Allosterism, Allosterically Regulated Targets, and Drug Discovery
When a screen and follow-up have failed to deliver an attractive lead for a 'hard' target, talk amongst the team often turns to running a screen for an allosteric inhibitor; Allosteric regulators are therefore a seductive/tantalising approach to find leads against tough targets such as protein-protein interactions, highly polar binding sites, etc.
But, there's a few hard questions to answer, this is just a few.
- Just how do I run a screen for an allosteric inhibitor?
- What compounds do I select for allosteric sites?
- How likely am I to find an allosteric inhibitor?
- What sorts of targets can be allosterically modulated?
- What are the 3-D properties of allosteric sites
I've read some of the literature behind the arguments for allosteric inhibitors, and I must say I'm not that convinced as to their general potential benefits at the moment - of course in some cases, they will be perfect, but are the advantages as general as people may think. But I've been wrong, so many times in my life by now, that it's always worth looking at the actual data. So, as part of the SMS-Drug project we're putting together (and here 'we' means Gerard) of an overview of allosteric binders within ChEMBL - hopefully leading to some annotation of the class of binding of compounds to their targets.
Here (below, click for larger), is an initial overview of the target classes from ChEMBL for which we find evidence of allosteric regulation - this is not the same as the a priori distribution of targets, and so it looks interesting.....
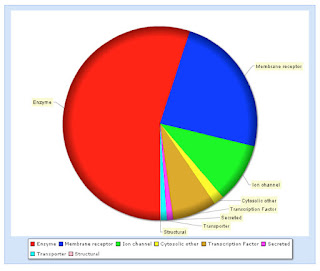 Hopefully, the full story of this analysis will appear in printed form reasonably soon.
Hopefully, the full story of this analysis will appear in printed form reasonably soon.
-
USAN Watch - July 2012
The USANs for July 2012 have recently been published.
USAN Research Code Structure Drug Class Therapeutic class Target avibactam, avibactam sodium NXL-104 
natural product-derived small molecule therapeutic beta lactamase insulin peglispro LY-2605541 protein therapeutic Insulin receptor rematercept ACE-031 protein therapeutic Myostatin sodium picosulfate 
synthetic small molecule therapeutic n/a