-
New Drug Approvals 2011 - Pt. XIII Linagliptin (TradjentaTM)

ATC code : A10BH05
On May 2nd, the FDA approved Linagliptin (BI-1356, trade name Tradjenta, ATC code A10BH05, ChEMBL ID 237500 NDA 201280), a dipeptidyl peptidase-4 (DPP-4) inhibitor, to treat type II diabetes (OMIM: 125853). Linagliptin has been approved for monotherapy or in combination with other medications, in conjunction with exercise and dietary modification. Due to a malfunction in production of or response to insulin, patients with type II diabetes suffer from high blood glucose levels.
By inhibiting DPP-4 (Uniprot P27487, OMIM: 102720, EC number 3.4.14.5), a cell surface glycoprotein receptor, Linagliptin stabilizes the level of two of its substrates, the intecrins GLP-1 and GIP, gastrointestinal peptide hormones which stimulate insulin release from beta cells of the Islets of Langerhans.
Linagliptin has been shown to have a high affinity (Ki 1 nM) for DPP-4 in cell-based fluorescence assays, and to be highly selective. DPP-4 exists in soluble form (aminoacids 39-766) or with a N-terminal single-anchor domain, linking the extracellular domain to the cell membrane. There are several homodimeric crystal structures available, e.g. PDB 1J2E. The -gliptin USAN stem covers DPP-IV inhibitors, and there are a number already launched (e.g. Saxagliptin, Sitagliptin and Vildagliptin) and many others in clinical trials/registration (e.g. Alogliptin (SYR-322, TAK-322), Carmegliptin (R-1579, Ro-4876904), Dutogliptin (PHX-1149), Gosogliptin (PF-734200), and Denagliptin (GSK-823903)). There are a very large number of others at earlier stages of development include R-1438, BI-1356, NVP-DPP-728, GRC-8200, SK-0403, P-32/98, PSN-9301, TS-021, R-1499, PSN-357, DP-893, LC-150444, BMS-686117, TAK-100, BMS-477128, ABT-279, ARI-2243, SSR-162339, ER-319711 Ro-0730699, NN-7201, MP-513, KRP-104, E-3024, and ALS-2-0426 (AMG-222).
The -gliptin USAN stem covers DPP-IV inhibitors, and there are a number already launched (e.g. Saxagliptin, Sitagliptin and Vildagliptin) and many others in clinical trials/registration (e.g. Alogliptin (SYR-322, TAK-322), Carmegliptin (R-1579, Ro-4876904), Dutogliptin (PHX-1149), Gosogliptin (PF-734200), and Denagliptin (GSK-823903)). There are a very large number of others at earlier stages of development include R-1438, BI-1356, NVP-DPP-728, GRC-8200, SK-0403, P-32/98, PSN-9301, TS-021, R-1499, PSN-357, DP-893, LC-150444, BMS-686117, TAK-100, BMS-477128, ABT-279, ARI-2243, SSR-162339, ER-319711 Ro-0730699, NN-7201, MP-513, KRP-104, E-3024, and ALS-2-0426 (AMG-222).
There is a previous ChEMBL-og monograph available for Saxagliptin.
Linagliptin (systematic name 8-[(3R)-3-aminopiperidin-1-yl]-7-(but-2-yn-1-yl)-3-methyl-1-[(4-methylquinazolin-2-yl)methyl]-3,7-dihydro-1H-purine-2,6-dione) has the chemical formula C25H28N8O2, molecular mass of 472.54 g/mol. ), AlogP of 2.1 and is fully Rule-of-five compliant.Smiles=CC#CCn1c(nc2N(C)C(=O)N(Cc3nc(C)c4ccccc4n3)C(=O)c12)N5CCC[C@@H](N)C5;InChI=1S/C25H28N8O2/c1-4-5-13-32-21-22(29-24(32)31-12-8-9-17(26)14-31)30(3)25(35)33(23(21)34)15-20-27-16(2)18-10-6-7-11-19(18)28-20/h6-7,10-11,17H,8-9,12-15,26H2,1-3H3/t17-/m1/s1.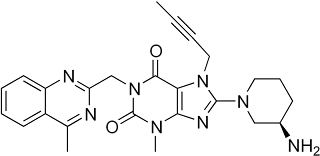
Tradjenta is dosed as a 5 mg tablet, once daily (equivalent to a daily dose of 10.6 umol).After a single administration, a maximum concentration (Cmax) of 8.9 nmol/L is reached after Tmax=1.5 h. Linagliptin has a long terminal half-life (>100 h) and steady-state plasma concentrations are reached after the third daily dose. At steady state, Cmax is increased by a factor of ~1.3 as compared to the single administration. The mean apparent volume of distribution (Vd) is approximately 1110 L.
Tradjenta is distributed by Boehringer Ingelheim and marketed by Boehringer Ingelheim and Eli Lilly and Company. In Europe the tradename is Trajenta. -
New Drug Approvals 2011 - Pt. XIV Boceprevir (VictrelisTM)

ATC code (partial): J
On May 13th, the FDA approved Boceprevir (Tradename: Victrelis; Research Code: SCH-503034, NDA202258), a Hepatitis C virus NS3 protease (HCV NS3) inhibitor, for the treatment of chronic hepatitis C virus genotype 1 infection, in combination with peginterferon alfa and ribavirin.
Chronic hepatitis C genotype 1 is a prolonged infection that affects the liver and is caused by a small single-stranded RNA virus, which is transmitted by blood-to-blood contact. Chronic hepatitis C is normally asymptomatic, but may lead to liver fibrosis, and thus liver failure.
Boceprevir is a first-in-class inhibitor of the hepatitis C virus (HCV) non-structural protein 3 (NS3) protease (ChEMBLID:CHEMBL4893; Uniprot ID:A3EZI9), a viral protein required for the proteolytic cleavage of the HCV encoded polyprotein (UniProt:P27958) into mature forms of the NS4A, NS4B, NS5A and NS5B proteins (NS3 is Uniprot: P27958[1027-1657]). These proteins are involved in the formation of the virus replication complex, and therefore are vital to its survival. HCV NS3 is a serine proteinase (Pfam:PF02907). Through a reactive center, the (alpha)-ketoamide functional group, boceprevir binds covalently to a serine in the active site of NS3 protease (S139), inhibiting viral replication in HCV-infected host cells. In a biochemical assay, Boceprevir inhibited the activity of recombinant HCV genotype 1a and 1b NS3/4A protease enzymes, with Ki values of 14 nM for each subtype.
There are many protein structures known for this protein in complex with inhibitors, a typical entry is PDBe:3rc4, as expected from early genome annotation, the NS3 proteinase has a fold distantly related to the chymotrypsin-like family of serine proteinases, and contains the classic Asp-His-Ser catalytic triad.
The -vir USAN/INN stem covers antiviral agents, and the substem -previr indicates it is a serine protease inhibitor. Boceprevir is the first approved agent to target HCV NS3. Other compounds in this class in late stage clinical development/registration include Vertex's Telaprevir (VX-950, Incivek), Tibotec's TMC-435, and Bristol Myers Squibb's Asunaprevir (BMS-650032). Others at earlier stages of development include ABT-450, BI-201335, IDX-320, MK-5172, Vaniprevir (MK-7009), Narlaprivir (SCH-900518), Danoprevir (RG-7227, ITMN-191), BIT-225, VX-500, ACH-1625, GS-9256, .

Boceprevir (IUPAC: (1S,4S,5R)-N-(4-amino-1-cyclobutyl-3, 4-dioxobutan 2-yl)-3-[(2S)-2-(tert-butylcarbamoylamino)-3, 3-dimethylbutanoyl]-6,6-dimethyl-3-azabicyclo[3.1.0]hexane-4-carboxamide; SMILES: CC1(C2C1C(N(C2)C(=O)C(C(C)(C)C)NC(=O)NC(C)(C)C)C(=O)NC(CC3CCC3)C(=O)C(=O)N)C; PubChem:10324367; ChEMBL ID: CHEMBL218394) is a 1:1 mixture of two diastereomers (SCH-534128 - active - and SCH-534129 - inactive). The inhibitor is clearly peptide like, containing three amino acid residues, mimicking the natural substrate of the protease. It has a molecular weight of 519.7 Da, contains 4 hydrogen bond donors, 5 hydrogen bond acceptors, and has an ALogP of 1.62.
Boceprevir is available as oral gelatin capsules of 200 mg. It has an apparent volume of distribution (Vd/F) of approximately 772 L, and, in patients who received a dose of 800 mg three times a day (the recommended daily dose is therefore a large 2.4 g (equivalent to 4,600 umol)), the exposure is characterised by an AUC of 5408 ng.hr/mL, a Cmax of 1723 ng/mL and a Cmin of 88 ng/mL. Boceprevir should be administered with food, since food enhances its bioavailability by up to 65%. Human plasma protein binding (ppb) is approximately 75% following a single dose of boceprevir of 800 mg.
The primary metabolising route of boceprevir is through the aldo-ketoreductase (AKR)-mediated pathway to ketone-reduced metabolites that are inactive against HCV (Pfam:PF00248). Boceprevir is eliminated with a mean plasma half-life (t1/2) of approximately 3.4 hours, and it has a mean total body clearance (CL/F) of approximately 161 L/hr.
Boceprevir is a strong inhibitor of CYP3A4, and therefore, other therapeutic agents primarily metabolised by these enzyme may prolong their therapeutic effect or adverse reactions, see prescribing information for the extensive list of drug-drug interactions, contraindications.
The license holder for Boceprevir is Merck & Co., and the full prescribing information can be found here. For more information, please visit the product website here. -
Kinase Inhibitors in Clinical Development

Here is a snapshot of the Clinical Development Phase kinase inhibitors we have identified, all 313 of them. Any feedback on the data would be great, so any missing compounds, mismapped synonyms, wrong highest phase data, etc. would really help tune our data discovery approaches for this sort of thing. Please do not send us any proprietary/licensed data that you are not free to share! -
ChEMBL User Group Meeting - Some Details
 The agenda for the first ChEMBL user group meeting is below, we also have some additional speakers on various collaborative projects likely to be of interest to attendees, as extra-meeting items. Many thanks to the speakers and to Brad Sherbourne of Merck for putting this together.
The agenda for the first ChEMBL user group meeting is below, we also have some additional speakers on various collaborative projects likely to be of interest to attendees, as extra-meeting items. Many thanks to the speakers and to Brad Sherbourne of Merck for putting this together.The presentations will be a mix of slides and generous discussion time, giving plenty of opportunity to shape the future development of ChEMBL.
Friday May 27th, Courtyard Meeting Room, EMBL-EBI, Hinxton, CB10 1SD.
9.15 Coffee/Reception
9.30 Welcome to ChUG - JPO and Brad
9.45 ChEMBL update and plans - ChEMBL group
10.45 Coffee
11.00 BeautifulBind: Prioritising targets by chemistry - Andrew Hopkins
11.45 Predicting targets using ChEMBL, and application to phospholipidosis - Rob Lowe
12.15 Lunch
13.15 QSAR workbench/Active learning - David Nicolaides
13.45 Matched-pair analysis, ChEMBL and KNIME - George Papadatos
14.15 Anti-Drugs - Willem Van Hoorn
14.45 Coffee
15.00 Comparison of compound to target mapping in ChEMBL and other databases - Chris Southan
15.30 Implementation/interface - Rich Hall
16.00 CanSAR - Mark Halling-Brown
16.30 Close of ChUG meeting
Extra Session
16.35 Stefan Senger - IMI OpenPHACTs Project
16.45 Mike Barnes - RSC Precompetitive activitiesThere is still time to register, details on the LinkedIn ChEMBL User Group. Travel details are on the EBI website www.ebi.ac.uk, when you arrive, present yourself to Security at the Campus Visitor Center, then you will be sent to the EBI reception where you'll be met and taken to the meeting room.
-
May 2011 USANs

The May 2011 USANs have been published.
USAN Research Code Structure Drug Type Drug Class Target alisertib, alisertib sodium MLN-8237 
synthetic small molecule therapeutic AURa, AURb asunaprevir BMS-650032 
synthetic small molecule therapeutic HCV NS3 cariprazine, cariprazine hydrochloride RGH-188 
synthetic small molecule therapeutic D2R D3R ceftolozane, ceftolozane sulfate CXA-101 
natural product-derived small molecule therapeutic various PBPs crenezumab MABT5102A monoclonal antibody therapeutic Abeta dalantercept ACE-041 
protein therapeutic TGFbeta family delcasertib, delcasertib acetate KAI-9803, BMS-875944 
peptide therapeutic PKCdelta epelsiban, epelsiban besylate GSK-557296B 
synthetic small molecule therapeutic Oxytocin receptor erismodegib LDE-225 
synthetic small molecule therapeutic Smo evacetrapib LY-2484595 
synthetic small molecule therapeutic CETP ficlatuzumab SCH-900105, AV-299 monoclonal antibody therapeutic HGF galeterone TOK-001, VN-124 
natural product-derived small molecule therapeutic AR icopasent ethyl AMR-101 
natural product-derived small molecule supplement - macitentan ACT-064992 
synthetic small molecule therapeutic ETRa ETRb oclacitinib, oclacitinib maleate PF-03394197 
synthetic small molecule therapeutic sarilumab REG-N88, SAR-153191 monoclonal antibody therapeutic IL6R sitaxentan sodium TBC-11251z, TBC-11251Na 
synthetic small molecule therapeutic ETRa ETRb tofacitinib citrate CP-690550-10 
synthetic small molecule therapeutic JAK2, JAK3 trametinib, trametinib dimethyl sulfoxide GSK-1120212 
synthetic small molecule therapeutic MEK volasertib, volasertib trihydrochloride BI-6727 
synthetic small molecule therapeutic PLK1 vonicog alfa BAX-111 
protein supplement
A fair few kinase inhibitors, but does anyone know anything about Oclacitinib - Google shows only some dog cancer trials at the moment? -
Recruitment: New Approaches to the Treatment of Cardiovascular Disease
 We are involved in a fascinating collaboration with Prof. Aroon Hingorani from the Clinical Epidemiology Dept of UCL Division of Medicine - working with clinical data to identify new approaches to the treatment of cardiovascular disease. Further details of the position are here. Closing date is May 23rd 2011 - so get your skates on!
We are involved in a fascinating collaboration with Prof. Aroon Hingorani from the Clinical Epidemiology Dept of UCL Division of Medicine - working with clinical data to identify new approaches to the treatment of cardiovascular disease. Further details of the position are here. Closing date is May 23rd 2011 - so get your skates on!
Behind the picture is a tale of woe.... -
ChEMBL Schema Walkthrough Webinar - 1st June 2011

We will be running another walkthrough of the ChEMBL database schema on Wednesday 1st June at 3pm BST (GMT+1).
-
The Office of Health Economics (OHE)
 One of my secret pleasures of the past used to be when the OHE published a new monograph on healthcare, I'd pick up a free copy from the library, and read it on the bus journey home. Often, they were connected to things like, QALYs and DALYs, which although interesting were not directly relevant to what I do; however, every now and then there was a real gem; for example, comparing structural differences between the UK and German biotech sectors, or re-costing the development costs of a new drug, or capturing the unexpected benefits on drug research (drug repurposing, etc). The monographs were great because they bought together scientific and healthcare innovation with well argued economic cases - a sort of science meets economics meets patients view, which is quite refreshing and rare.
One of my secret pleasures of the past used to be when the OHE published a new monograph on healthcare, I'd pick up a free copy from the library, and read it on the bus journey home. Often, they were connected to things like, QALYs and DALYs, which although interesting were not directly relevant to what I do; however, every now and then there was a real gem; for example, comparing structural differences between the UK and German biotech sectors, or re-costing the development costs of a new drug, or capturing the unexpected benefits on drug research (drug repurposing, etc). The monographs were great because they bought together scientific and healthcare innovation with well argued economic cases - a sort of science meets economics meets patients view, which is quite refreshing and rare.
The OHE went quiet for a few years (for me at least), but on the new website www.ohe.org there are a bunch of cool, free things from a drug discovery perspective. A good example is the monograph on New Drugs To Tackle Antimicrobial Resistance.






