-
World Malaria Day 2011

World Malaria Day for 2011 is on April 25th again this year - see the worldmalariaday website for more details. Also look at the ChEMBL-NTD website for some relevant data from the ChEMBL resources. -
Drug combinations as a possible approach to minimization of side effects?

I'm writing a foreword for a book on drug side effects, and thought of something that doesn't really fit in with the theme of the book, and so thought I would post it here (I'd better get a free copy of the book when it comes out, or the foreword will be really bad ;) ). Combination drugs are quite common, and typically contain agents that target different processes in the same pathway (there is a database DCDB that records a wide range of therapeutically used drug combinations if you're interested in seeing some real examples), there a have also been a few biotechs that have searched for synergistic (sometimes referred to as potentiating) combinations of drugs, foremost has to be CombintoRx (again have a click around their website for an idea of their approach).
However, what about thinking about co-dosing me-too drugs as a rational way to minimise side effects. By this I mean taking two different statins, or two alpha-antagonists (there's nothing special about these targets or drugs, they just sprang to mind while writing; and of course it may not need to be two, it could be three or four....) and co-dosing them. So assuming in the first instance that they have similar PK properties, and imagine that they have a 100 mg once daily dosing scheme, and furthermore, suspend reality and pretend they have identical potency against their therapeutic target - remember this is a thought experiment after all. The idea would be to combine them in a new pill with 50 mg of each component. This would minimize side effects through a really simple mechanism....
Drugs are not selective, they interact with many, usually tens, but maybe sometimes hundreds, of proteins in the body at clinical concentrations. The higher the Cmax of a drug, the more targets will be affected (so, think about drugs having an activity spectrum, analogous to a classical energy spectrum - the more energy available (equivalent to the concentration of the drug) the more ernergy states will be populated (targets will be affected)). So the higher the concentration of a drug, the more likely side effects are likely to occur (in fact it is well established that most adverse events are associated with peaks in free drug concentration). So two drugs targeting the same target can be combined to achieve an equivalent coverage of the receptor/enzyme. However the Cmax for each drug will be lower, and since the binding to off-targets will likely be different for the two drugs, halving the dose of each component would halve the Cmax for each drug and should greatly minimize the likelihood of adverse events. A key assumption here is that there are different binding profiles for the drugs, this seems a reasonable assumption, and it would be possible to explore this idea, if one had access to the data. However, even if they are identical in binding profile, it cannot be more dangerous with respect to off target side effects, than dosing with a single agent. The optimal combinations would have uncorrelated activity profiles, other than sharing similar affinity for their efficacy target.
Some negatives for this scheme include an increased chance of reaction to a drug containing a mixture of two (or more) active components, secondly, co-dosing drugs that interfered with, or saturated, the others metabolism is bound to lead to trouble, and thirdly, the business benefits of implementing this aren't obvious. Anyway, does anyone know of any attempts to try this idea in patients? One that occurs to me is the parallel dosing with COX inhibitors (paracetamol, ibuprofen and aspirin), but are there any other examples. -
Registration now open for the ChEMBL User Group (ChUG) meeting
 Registration is now open on the LinkedIn ChEMBL User Group page for our first meeting. If you are not on LinkedIn and would still like to come, please mail me.
Registration is now open on the LinkedIn ChEMBL User Group page for our first meeting. If you are not on LinkedIn and would still like to come, please mail me.
To parents of young children the world over (in 175 territories in fact) the image above will be too familiar. -
New Drug Approvals 2011 - Pt. IX Ipilimumab (YervoyTM)

ATC code:L01XC11
Malignant melanoma is diagnosed in an estimated 160,000 new patients each year and, despite being less common than other skin neoplasms, it is responsible for 75% of skin cancer-related deaths. Current available treatment options for melanoma are limited to surgery, chemotherapy, radiotherapy and immunotherapy, although there are a number of targetted agents in the clinical development at the moment. Ipilimumab effect in melanoma is indirect and probably due to enabling a T-cell mediated immune responseIn a randomised clinical study that assessed the response of unresectable or metastatic melanoma patients to Ipilimumab, alone and in combination with investigational peptide vaccine adjuvant, gp100, the combination showed increased survival time (median survival of 10 months, compared with 6.4 months for patients receiving the vaccine alone) as well as a near doubling of the rates of survival at 12 months (46% vs 25%) and 24 months (24% vs 14%) as compared to the peptide alone.
Ipilimumab's molecular target is CTLA-4 (Uniprot: P16410; canSAR ; PFAM: P16410), a negative regulator of T-cell activation. Ipilimumab augments T-cell activation and proliferation by binding to CTLA-4 and preventing its interaction with its ligands (CD80 and CD86). CTLA-4 is a membrane-bound, 223 amino acid long, T-cell protein. It contains an immunoglobulin V-type domain (PFAM:PF07686). The structure of CTLA-4 is determined (see e.g. PDBe:3osk) Ipilimumab has been issued with a Black Box warning as it can result in severe and fatal immune-mediated adverse reactions due to T-cell activation and proliferation, particularly enterocolitis, hepatitis, dermatitis (including toxic epidermal necrolysis), neuropathy, and endocrinopathy.
Ipilimumab has been issued with a Black Box warning as it can result in severe and fatal immune-mediated adverse reactions due to T-cell activation and proliferation, particularly enterocolitis, hepatitis, dermatitis (including toxic epidermal necrolysis), neuropathy, and endocrinopathy.
Ipilimumab is administered intravenously, and the recommended dose is 3 mg/kg administered over 90 minutes every 3 weeks for a total of four doses. The terminal half-life (t1/2) is 14.7 days (30.1%); systemic clearance (CL) is 15.3 mL/h (38.5%); and volume of distribution at steady-state (Vss) is 7.21 L (10.5%).
The full prescribing information can be found here. Yervoy™ is a product of Bristol-Myers Squibb
-
GPCR Structures - Agonist form of A2a PDBe:3QAK
 There is a new GPCR structure available, an engineered form of human A2a complexed with an agonist ligand, the Phase 2 clinical candidate UK-432,097 (PDBe:3QAK). The paper accompanying this structure is available on the Science website.
There is a new GPCR structure available, an engineered form of human A2a complexed with an agonist ligand, the Phase 2 clinical candidate UK-432,097 (PDBe:3QAK). The paper accompanying this structure is available on the Science website.
UK-432,097
%T Structure of an Agonist-Bound Human A2A Adenosine Receptor %A Xu F %A Wu H %A Katritch V %A Han GW %A Jacobson KA %A Gao ZG %A Cherezov V %A Stevens RC %J Science %D 2011 %O PDBe:3qak %O DOI:10.1126/science.1202793
I've also updated the GPCR page with all the recent structures (there were some new beta-1 and beta-2 structures as well). -
A UK Academic Network for Chemical and Structural Biology in Drug Discovery

This Network will establish an Academia-Users Network in Chemical Biology to initiate, establish and nurture collaborative projects for the advancement of the drug discovery process. It aims to expand the capability of UK drug discovery, with new drug targets, new tools to validate targets and new multidisciplinary partnerships to explore the platforms, tools and targets of the future.
A poster for this new network is above, but a website is being set-up for this, and as soon as it is ready to go, we'll provide links on the ChEMBL-og.
The network is funded by the EPSRC, BBSRC and MRC, funded through their joint “Collaborative Networks in Chemical Biology” initiative. -
Conference: 4ECCLS, Budapest, August 31-September 3 20117 2011
There's a great looking conference in Budapest this August, the 4th European Conference on Chemistry for Life Sciences (4ECCLS) - a link to the conference website is http://www.4eccls.mke.org.hu/ -
A Taxonomy for Drugs: 3 - Antibody subtypes

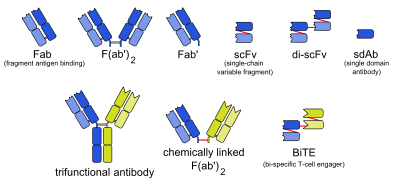
There is an excellent description of specific subtypes of monoclonal antibodies on Wikipedia, these can be easily incorporated into the Drug_Class section of our drug taxonomy. Specifically as Drug_Type_Subsubclass. An interesting property of this classification is that it should be possible to write an algorithm that classifies arbitrary sequences against this taxonomy.
- mab - whole monoclonal antibody.
- Fab - fragment, antigen-binding (one arm).
- F(ab')2 - fragment, antigen-binding, including hinge region (both arms).
- Fab' - fragment, antigen-binding, including hinge region (one arm).
- scFv - single-chain variable fragment.
- di-scFv - dimeric single-chain variable fragment.
- sdAb - single-domain antibody.
- 3funct - trifunctional antibody.
- BiTE - bi-specific T-cell engager.
- Other - an antibody like drug that does not fit one of the above classes.