On February 28th, 2011, the FDA approved Roflumilast (tradename:Daxas tradename:Daliresp NDA 022522) for the treatment of patients with chronic obstructive pulmonary disease (COPD) a chronic and serious disease involving restriction of full lung function. The narrowing of airways of COPD is irreversible, and follows inflammation in the lung, believed to be linked to environmental pollutants such as tobacco smoke, workplace dusts and urban air pollution. This inflammation causes structural damage to the delicate alveoli structures.
Roflumilast and an active metabolite, Roflumilast-N-Oxide, are selective Phosphodiesterase 4 inhibitors. The subfamily of Type 4 Phospodiesterases comprises four distinct members, PDE4A, -4B, -4C, and -4D (Uniprot:P27815, Q07343, Q08493, Q08499, respectively, all are very closely related enzymes containing a characteristic cyclic nucleotide diesterase catalytic domain Pfam:PF00233). These in turn occur in different splicing isoforms with tissue specific expression, many of them in the lung. Phosphodiesterase 4 catalyzes a reaction transforming cyclic 3'-5'-adenosine monophosphate (cAMP, ChEBI: 17489) into adenosine 5'-monophosphate (AMP). Roflumilast has an IC50 against PDE-4 of ca. 2nM, affinities against the PDE4A, PDE4B, and PDE4D isozymes are all similar, whereas affinity against the PDE4C isozyme is ca. 5 fold lower. The exact mechanism by which Roflumilast reduces the risk of COPD exacerbations is not known, but it is believed that an increase in cAMP levels in lung cells attenuates the abnormal inflammation process associated with COPD. In clinical trials, it was observed that the numbers of specific types of immune cells - eosinophils and neutophils - were reduced by 31% and 42% after 4 weeks of treatment with Roflumilast.
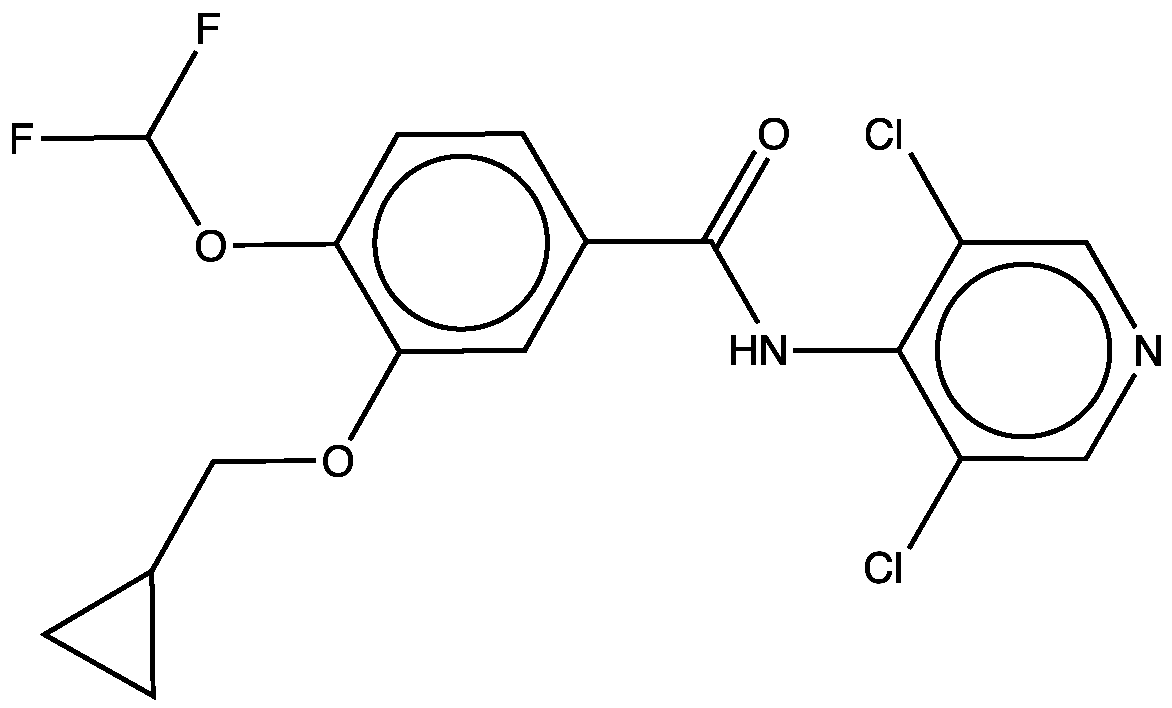
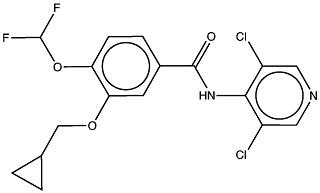
Roflumilast ( IUPAC: 3-(cyclopropylmethoxy)-N-(3,5-dichloropyridin-4-yl)-4-(difluoromethoxy)benzamide InChI: 1S/C17H14Cl2F2N2O3/c18-11-6-22-7-12(19)15(11)23-16(24)10-3-4-13(26-17(20)21)14(5-10)25-8-9-1-2-9/h3-7,9,17H,1-2,8H2,(H,22,23,24) SMILES: FC(F)Oc1ccc(cc1OCC2CC2)C(=O)Nc3c(Cl)cncc3Cl Chemspider:395793 ChEMBL:193240) is a synthetic small molecule drug containing no chiral centers. It has a molecular weight of 403.2 Da and calculated LogP of 4.4. Roflumilast has 4 hydrogen bond acceptors and 1 hydrogen bond donor and therefore fully complies with Lipinski's rule of five.
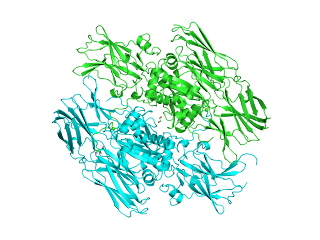
The structure of a number of phosphodiesterase enzymes are known, including a number of PDE4 isoforms, a typical complex of PDE4D with an inhibitor is PDBe:1y2k
Roflumilast's oral bioavailability (at the recommended dose of 500 ug) is approximately 80% and the volume of distribution (Vd) is about 2.9 L.kg-1 and a clearance (CL) of 9.6 L.hr-1. Roflumilast is transformed into an active metabolite, Roflumilast-N-oxide via a metabolic route involving cytochromes CYP1A2 (Uniprot: P05177) and CYP3A4 (Uniprot: P08684). It is the only metabolite observed in humans at relevant plasma concentrations. In-vitro inhibition of Phosphodiesterase 4 by the active metabolite is three times less potent compared to the parent compound. However, its plasma AUC is about 10-fold greater than the plasma AUC of Roflumilast. Maximum plasma concentrations CMAX of Roflumilast and Roflumilast-N-oxide are reached after 1 hour and eight hours, respectively. Plasma protein binding (ppb) of the dosed drug and the active metabolite is 99% and 97% respectively. Roflumilast is eliminated primarily through the urine and the drug's half life after oral administration is 17 hours and 30 hours for Roflumilast-N-oxide.
Roflumilast is administered once daily as an oral tablet containing 500 ug of active ingredient (equivalent to 1.2 umol).
The full prescribing information can be found here.
Roflumilast was approved by the European commission in 2010 and is marketed in Europe as Daxas. In the US, Roflumilast will be marketed by Forest Pharmaceuticals under the trade name Daliresp (product website).
The deadline for applications for the 2011 intake for EIPODs (interdisciplinary postdoc fellowships within EMBL, funded by EMBL and Marie Curie Actions) is approaching soon - 20th March 2011 to be specific. There are lots of interesting predefined projects, but also the opportunity to define your own collaborative project between EMBL faculty in different units.
The ChEMBL group are involved in two predefined projects 1) NGS methods for natural product profiling/discovery and 2) text mining approaches for clinical candidate discovery from the literature.
The most recent FDA drug approval is Azilsartan Medoxomil, approved on February 25th (NDA 200796). Azilsartan Medoxomil (research code: TAK-491; tradename: Edarbi) is an angiotensin II receptor blocker prodrug indicated for the treatment of hypertension, either alone or in combination with other antihypertensive agents. Hypertension is a medical condition in which the blood pressure in the vessels is too high, and can lead to kidney failure, stroke, myocardial infarction (heart attack), aneurysm, and many other pathologies. The renin-angiotensin system is a key regulator of blood pressure; Angiotensin is an hormone system that regulates the blood pressure and the fluid balance. The short peptide Angiotensin II is the principal agent of this system, and is responsible for vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac stimulation, and renal reabsorption of sodium.
Azilsartan (ChEMBL: ChEMBL57242; PubChem: CID9825285; Chemspider: 8001032), the bioactive ingredient of the prodrug Azilsartan Medoxomil, is a selective AT1 subtype angiotensin II receptor (ChEMBL: ChEMBL227; Uniprot: P30556) antagonist and exerts its therapeutic effects by selectively blocking the binding of angiotensin II to the AT1 receptor in tissues, such as vascular smooth muscle and the adrenal gland. Angiotensin receptors are a class of G protein-coupled receptors (GPCR) that belong specifically to the family of rhodopsin-like receptors and in which the drug binding occurs at a well defined site within the ligand-binding domain (PFAM: PF00001). A second angiotensin receptor is also known - AT2 angiotensin II receptor (ChEMBL: CHEMBL4607; Uniprot: P50052) which is broadly expressed and suggested to mediate effects such as inhibition of cell growth, fetal tissue development, modulation of extracellular matrix, neuronal regeneration, apoptosis, cellular differentiation. AT2 angiotensin II receptor is not known to be associated with cardiovascular homeostasis and, moreover, Azilsartan has more than 10k-fold greater affinity for the AT1 receptor (with an IC50 of 2.6 nM for human AT1 receptor) than for the AT2 receptor. Also, Azilsartan does not significantly bind or block other receptors or ion-channels known to be involved in cardiovascular regulation.
Several treatments for hypertension are already in the market and these include, not only treatments with other angiotensin II receptor antagonists, such as Olmesartan Medoxomil (approved in 2002; tradename: Benicar), but also treatments with ACE inhibitors (e.g. Enalapril, approved in 1985; tradename: Vasotec), alpha-blockers (e.g. Prazosin, approved in 1976; tradename: Minipress), beta-blockers (e.g. Nebivolol, approved in 2007; tradename: Bystolic), calcium channel blockers and direct renin inhibitors (e.g. Aliskiren, approved in 2007; tradename: Tekturna). The -sartan USAN/INN stem covers angiotensin II receptor antagonists; other approved -sartan drugs from the C09CA ATC class include Candesartan, Eprosartan, Irbesartan, Losartan, Tasosartan, Telmisartan, and Valsartan. Sartans are often dosed with other antihypertension medications as a combination therapy.
Azilsartan Medoxomil (IUPAC: (5-methyl-2-oxo-1,3-dioxol-4-yl)methyl-2-ethoxy-3-[[4-[2-(5-oxo-1-oxa-2-aza-4-azanidacyclopent-2-en-3-yl)phenyl]phenyl]methyl]benzimidazole-4-carboxylate; SMILES: O=C(C1=C2C(N=C(OCC)N2CC3=CC=C(C4=CC=CC=C4C(N5)=NOC5=O)C=C3)=CC=C1)OCC6=C(C)OC(O6)=O ) has a molecular weight of 568.53 Da (606.62 Da for the potassium salt), has 1 hydrogen bond donor, 10 hydrogen bond acceptors, an AlogP of 5.3, a polar surface area of 139.6 Å2 and 10 rotatable bonds, which makes the molecule very flexible. Azilsaratan Medoximil does not contain any chiral centers, and as the active drug azilsartan, the physicochemistry will be dominated by the negatively charged carboxylic acid. Azilsartan medoximil is a synthetic small molecule drug.
Azilsartan Medoxomil is available for oral use as tablets. Each tablet contains 40 mg and 80 mg of Azilsartan Medoxomil. At the 80 mg dose level used in Edarbi, the daily molar dose is 140.7 µmol. Azilsartan Medoxomil is hydrolyzed to Azilsartan, the active metabolite, in the gastrointestinal tract during absorption. Azilsartan is relatively poorly absorbed (60% bioavailability), a volume of distribution (Vd) of approximately 16 L and a high plasma protein binding of >99%. Azilsartan is metabolised, mainly by CYP2C9, to two primary metabolites: a major metabolite formed by O-dealkylation, and a minor metabolite, formed by decarboxylation. These metabolites do not contribute to the pharmacologic activity of Azilsartan Medoxomil. Azilsartan Medoxomil is recovered in both feces (55%) and urine (42%), with 15% of the dose being excreted in urine as Azilsartan. The elimination half-life (t1/2) of Azilsartan is ca. 11 hours and the renal clearance (CL) is ca. 2.3 mL.min-1.
Azilsartan Medoxomil has a black box warning - and should not be used in pregnancy.
The full prescribing information can be found here.
We are collaborators on a paper just published in Nature Reviews Drug Discovery, investigating the relationship of in vitro and physicochemical data and ADMET properties, as you will imagine, a lot of the underlying data for this work and analysis came from the ChEMBL database. There is quite a lot of new stuff in there...
%J Nature Reviews Drug Discovery
%V 10
%P 197-208
%D 2011
%O doi:10.1038/nrd3367
%T Probing the links between in vitro potency, ADMET and physicochemical parameters
%A M.P. Gleeson
%A A. Hersey
%A D. Montanari
%A J. Overington
We are pleased to announce the release of the ChEMBL RESTful Web Service API (application programming interface). The first release provides the functionality to support programmatic retrieval of ChEMBLdb compound, target, assay, and bioactivity data. In the coming weeks and months we will extend the feature set of the REST API to support:
Searching of compounds with SMILES, InChI keys, including substructure and similarity searches
Searching of targets by protein identifiers
Retrieval of results in JSON format
We have provided a documentation page that describes the API functionality in more detail and also describes how to get started with using our java client to access API: https://www.ebi.ac.uk/chembldb/index.php/ws.
As always, you're feedback and suggestions for improving the API are most welcome. Please e-mail: chembl-help@ebi.ac.uk.
Update: In answer to an email question, the API is secure, runs under https: (http: calls will automatically be redirected automatically). The usual EBI terms of use apply to these services.
On February 17th 2011, the FDA approved human coagulation Factor XIII (FXIII) Concentrate as an orphan drug under the trade name Corifact (ATC code B02BD07) to treat congenital Factor XIII deficiency (OMIM:134570 and OMIM:134580, ICD-10:D68.2). The incidence of this rare condition is 1 in 1 to 5 million, making it the rarest form of hemophilia. The genetic deficiency leads to defective fibrin crosslinking, the terminal step of the coagulation cascade which leads to blood forming clots to deplete its loss from damaged vessels.
Prior to US approval, FXIII Concentrate had already been marketed in Europe, as Fibrogammin P, developed by CSL Behring of Marburg, Germany. Recently, recombinant FXIII (rFXIII, Novo Nordisk, Bagsværd, Denmark) has completed phase 3 clinical trials.
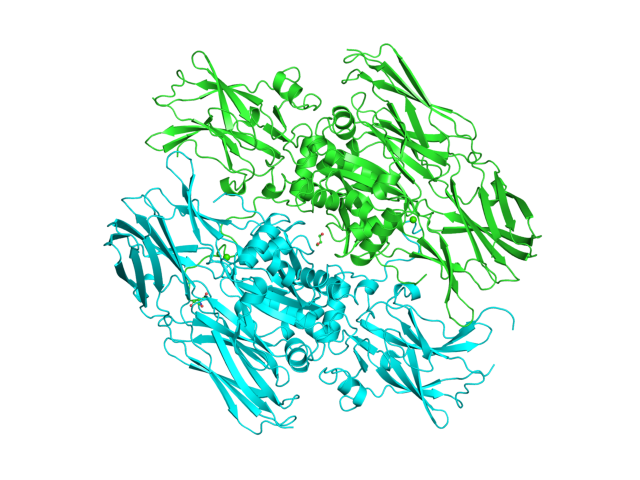
FXIII exists naturally as a secreted, tetrameric protein (with composition A2B2) with a molecular weight of ca. 320 kDa. The tetramer consists of twice two catalytically active transglutaminase (A subunit, Uniprot:P00488) (E.C. 2.3.2.13) and an enzymatically inactive carrier (B subunit, Uniprot:P05160) subunits in the blood plasma, or as a catalytically active dimer (A2) inside platelets, monocytes, macrophages and their respective precursor cells. The B-chain holds the A chain dimer in an inactive state, and also shields the A-chain from proteolytic degradation in the plasma.
Several crystal structures are available for the catalytically active A chain dimer of FXIII, e.g. PDBe:1EVU.
FXIII is activated by proteolytic cleavage of the first 37 N-terminal amino acids by thrombin (also known as factor II). In presence of calcium ions, the carrier subunits dissociate, leading to a conformational change exposing the catalytic center of the A chain, thus capable of crosslinking of fibrin molecules to form an insoluble clot. In order to restore natural coagulaton, patients suffering from FXIII deficiency can therefore be treated with exogenous FXIII.
The half-life (t1/2) of Corifact is 6.6 days, with a steady state Volume of distribution (Vss) of 52 mL.kg-1, and a Clearance (Cl) of 0.25 mL.hr-1.kg-1.
Corifact is made from pooled human donor blood plasma, and is supplied as lyophilized concentrate for intravenous administration after reconstitution with sterile water. The recommended initial dosing is specific to the patients body weight and existing blood coagaultion parameters. Typical dosage is 40 IU per kg body weight and is repeated every 28 days. In the subsequent dosing, FXIII activity levels are monitored, and adjusted to achieve the intended trough FXIII activity level. As a human blood product, the production process of Corifact is monitored to minimize possible contamination with virus (e.g., HIV, HAV, HBV, and HCV), and the infective agent of CJD.
The full prescribing information can be found here.
The license holder for Corifact is CSL Behring, and the product website is here.
Thanks to Yumi for the translation of our ChEMBL home page into Chinese. At the moment, this is on the dev site http://wwwdev.ebi.ac.uk/chembl, but it will soon migrate to the normal location.


 Roflumilast's oral bioavailability (at the recommended dose of 500 ug) is approximately 80% and the volume of distribution (Vd) is about 2.9 L.kg-1 and a clearance (CL) of 9.6 L.hr-1. Roflumilast is transformed into an active metabolite, Roflumilast-N-oxide via a metabolic route involving cytochromes CYP1A2 (Uniprot: P05177) and CYP3A4 (Uniprot: P08684). It is the only metabolite observed in humans at relevant plasma concentrations. In-vitro inhibition of Phosphodiesterase 4 by the active metabolite is three times less potent compared to the parent compound. However, its plasma AUC is about 10-fold greater than the plasma AUC of Roflumilast. Maximum plasma concentrations CMAX of Roflumilast and Roflumilast-N-oxide are reached after 1 hour and eight hours, respectively. Plasma protein binding (ppb) of the dosed drug and the active metabolite is 99% and 97% respectively. Roflumilast is eliminated primarily through the urine and the drug's half life after oral administration is 17 hours and 30 hours for Roflumilast-N-oxide.
Roflumilast's oral bioavailability (at the recommended dose of 500 ug) is approximately 80% and the volume of distribution (Vd) is about 2.9 L.kg-1 and a clearance (CL) of 9.6 L.hr-1. Roflumilast is transformed into an active metabolite, Roflumilast-N-oxide via a metabolic route involving cytochromes CYP1A2 (Uniprot: P05177) and CYP3A4 (Uniprot: P08684). It is the only metabolite observed in humans at relevant plasma concentrations. In-vitro inhibition of Phosphodiesterase 4 by the active metabolite is three times less potent compared to the parent compound. However, its plasma AUC is about 10-fold greater than the plasma AUC of Roflumilast. Maximum plasma concentrations CMAX of Roflumilast and Roflumilast-N-oxide are reached after 1 hour and eight hours, respectively. Plasma protein binding (ppb) of the dosed drug and the active metabolite is 99% and 97% respectively. Roflumilast is eliminated primarily through the urine and the drug's half life after oral administration is 17 hours and 30 hours for Roflumilast-N-oxide.


 We are collaborators on a paper just published in Nature Reviews Drug Discovery, investigating the relationship of in vitro and physicochemical data and ADMET properties, as you will imagine, a lot of the underlying data for this work and analysis came from the ChEMBL database. There is quite a lot of new stuff in there...
We are collaborators on a paper just published in Nature Reviews Drug Discovery, investigating the relationship of in vitro and physicochemical data and ADMET properties, as you will imagine, a lot of the underlying data for this work and analysis came from the ChEMBL database. There is quite a lot of new stuff in there...